Telehealth and RPM billing have become central to how modern practices generate and protect revenue. Whether you operate a small primary care office or manage a multi-specialty group, virtual care billing now touches nearly every part of your revenue cycle. Getting it wrong — even on a single modifier or place of service code — can trigger claim denials that cost your practice thousands of dollars per month. At TMS Billings, our Revenue Cycle Management Services team works with practices across the country to recover lost telehealth revenue and build billing workflows that consistently get paid. This guide covers everything your team needs to know for 2026.
What Is Telehealth and RPM Billing in 2026?
What Is Telehealth and RPM Billing? Telehealth and RPM billing is the process of coding, submitting, and collecting payment for virtual care visits and remote patient monitoring services. It involves selecting the correct CPT codes, modifiers, and place of service codes required by Medicare, Medicaid, and commercial payers to support reimbursement for care delivered outside a traditional office setting.
Telehealth billing covers real-time video visits, audio-only appointments, asynchronous telehealth, and a growing range of remote monitoring services. Remote patient monitoring billing — specifically — refers to the collection and clinical review of physiological data from patients using connected devices between visits.
In 2026, telehealth and RPM billing operate under a more structured regulatory framework than during the pandemic years. CMS has extended many temporary flexibilities and codified key provisions permanently, but the rules still require careful attention to:
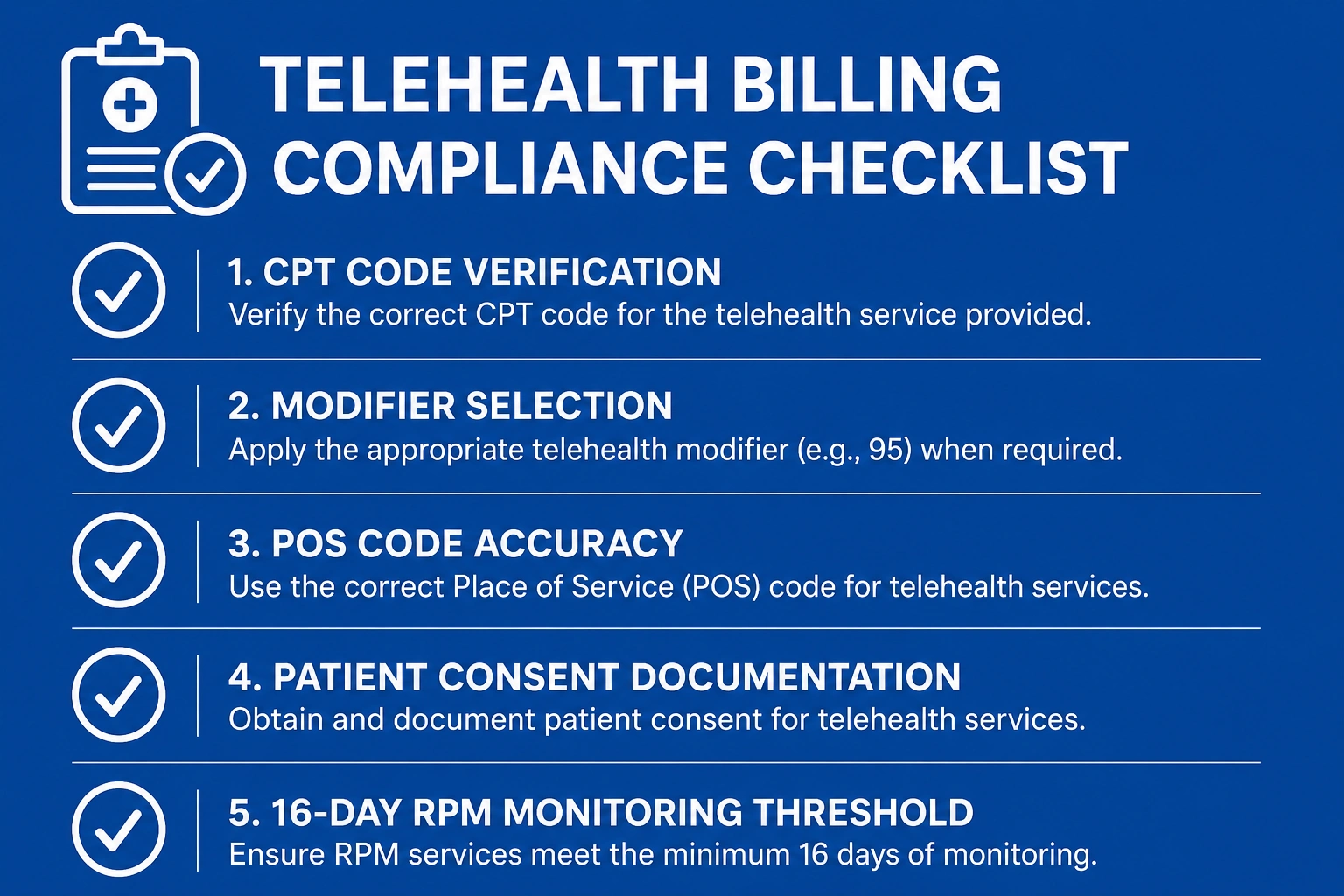
- CPT code selection
- Place of service (POS) codes
- Telehealth modifiers (95, GT, GQ)
- Patient eligibility
- Documentation requirements
If your practice offers any form of virtual care — from a single video follow-up to a full chronic care RPM program — you need a billing workflow that matches the complexity of the service being delivered.
Why Telehealth and RPM Billing Is Now a Revenue Priority for Every Practice
Virtual care is no longer a temporary accommodation. It is a permanent part of how patients access healthcare — and a permanent billing responsibility for your team.
What Changed in Telehealth Billing After the COVID-19 Flexibilities Ended
During the public health emergency (PHE), CMS waived many telehealth restrictions. Practices could bill from any location, see patients anywhere, and use audio-only platforms without penalty. When the PHE ended, some of those flexibilities expired — and practices that had built their workflows around emergency rules found themselves suddenly out of compliance.
The most significant post-PHE changes included:
- Restoration of originating site requirements for some telehealth services
- Narrowing of audio-only billing eligibility for certain E/M visits
- Reinstatement of geographic restrictions for specific Medicare telehealth categories
Practices that did not update their billing processes after the PHE wound down experienced a spike in claim denials — some of which went undetected for months.
CMS Telehealth Coverage Extensions and What’s Permanent in 2026
CMS has continued to expand its list of covered telehealth services. The 2026 Medicare Physician Fee Schedule telehealth provisions confirm several permanent extensions, including:
- Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) as eligible distant sites
- Expanded behavioral health telehealth access with in-person visit requirements waived for certain populations
- Continued coverage for mental health services delivered via audio-only when video is not feasible
Practices should verify their specific service lines against the CMS telehealth covered services list annually, as covered codes are updated each plan year.
Why Many Practices Are Still Leaving RPM Revenue on the Table
Remote patient monitoring billing offers a significant recurring revenue stream for primary care, cardiology, endocrinology, and other chronic disease management specialties. Yet many practices either do not bill for RPM at all or bill it incorrectly.
Common reasons practices lose RPM revenue:
- Failure to document the 16 minimum monitoring days required under CPT 99454
- Incomplete patient consent documentation at RPM enrollment
- Billing 99457 without adequate time documentation for the clinical review
- Confusing RPM with Remote Therapeutic Monitoring (RTM) — two distinct billing pathways with different eligible providers and CPT codes
The Hidden Revenue Risk of Incorrect Telehealth Billing
A single modifier error on a telehealth claim does not just deny that one claim. In many cases, payers retroactively audit all claims sharing the same billing pattern, resulting in recoupment requests that cover months of services. The financial exposure from systemic telehealth billing errors is significantly higher than most practice managers realize — and it often surfaces during a routine audit rather than a targeted inquiry.
The Biggest Causes of Telehealth and RPM Billing Denials in 2026
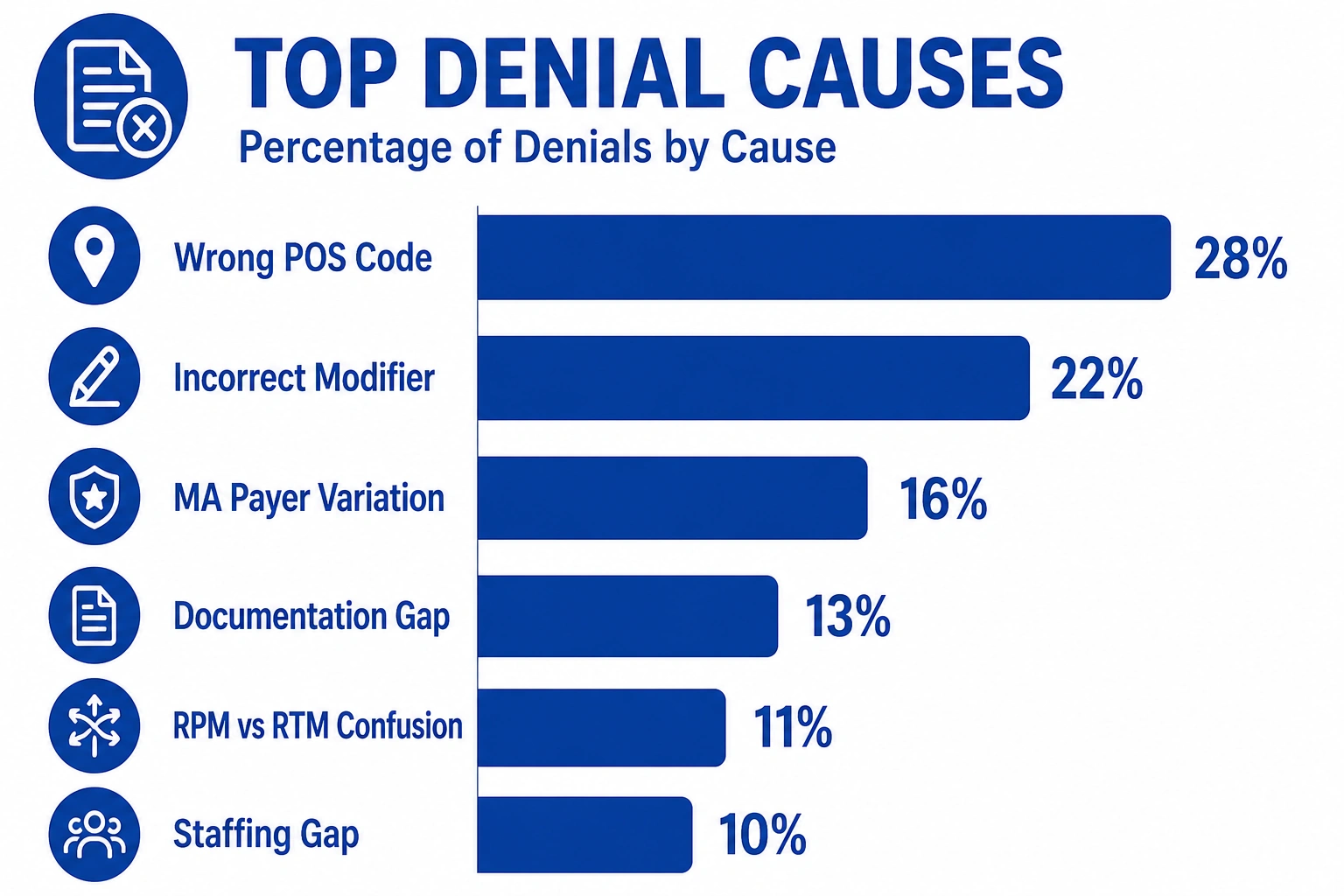
Understanding why claims get denied is the first step toward preventing them. The TMS Billings revenue cycle team has identified six recurring denial patterns specific to virtual care billing.
Using the Wrong Place of Service (POS) Codes
Place of service codes tell payers where the service was delivered. For telehealth, the two most commonly used codes are:
- POS 02 — Telehealth service provided in a setting other than the patient’s home
- POS 10 — Telehealth service provided in the patient’s home
Submitting a telehealth claim with POS 11 (Office) without the appropriate modifier communicates to the payer that the visit happened in person. If the payer’s records indicate otherwise, the claim will be denied or flagged for audit.
Missing or Incorrect Telehealth Modifiers (95, GT, GQ)
Modifiers communicate the nature of the service to the payer. The three primary telehealth modifiers are:
| Modifier | Use Case |
|---|---|
| 95 | Synchronous real-time telehealth via interactive audio and video — standard for commercial payers |
| GT | Interactive audio and video telehealth — used for traditional Medicare claims |
| GQ | Asynchronous (store-and-forward) telehealth services |
Using GT on a commercial payer claim that requires 95 — or omitting the modifier entirely — are among the most consistent causes of denial in telehealth billing 2026.
Medicare Advantage Payer Variation in Virtual Care Coverage
Medicare Advantage (MA) plans are not required to follow traditional Medicare telehealth rules. Each plan sets its own prior authorization requirements, covered codes, and reimbursement rates for virtual care. A practice billing telehealth for both traditional Medicare and MA patients using the same modifier and POS combination will almost certainly see denials on the MA side.
Documentation Gaps That Trigger Automatic Denials
Telehealth visits must be documented as thoroughly as in-person visits. In addition to standard E/M requirements, telehealth billing compliance demands:
- A statement confirming the visit was conducted via telehealth
- Documentation of the patient’s location at time of service
- Confirmation of patient consent (required for audio-only visits under Medicare)
- The technology platform used, if required by specific payers
Confusing RPM With Remote Therapeutic Monitoring (RTM)
RPM and RTM are related but distinct billing pathways. Billing RPM codes for services that qualify as RTM — or vice versa — is both a compliance risk and a denial trigger.
| Feature | RPM | RTM |
|---|---|---|
| Data type | Physiological (BP, glucose, weight, O2) | Therapeutic (pain, adherence, function) |
| Who can bill | Physicians and qualified NPPs | Expanded to PTs, OTs, SLPs |
| Key CPT codes | 99453, 99454, 99457, 99458 | 98975, 98976, 98977, 98980, 98981 |
Staffing Gaps in Telehealth Claims Follow-Up
Many practices do not have dedicated billing staff trained specifically in telehealth reimbursement. When denials occur, they often sit in the queue too long, pushing them past the timely filing limit. Leveraging Medical Billing Services from a team with specific virtual care expertise can close that gap before it becomes a revenue problem.
The Complete CPT Code Guide for Telehealth and RPM Billing
Accurate CPT code selection is the foundation of any successful telehealth reimbursement strategy.
Telehealth Visit CPT Codes (E/M and Behavioral Health)
Standard office E/M codes (99202–99215) are used for telehealth visits when billed with the appropriate modifier and POS code. Behavioral health codes — including 90832, 90834, and 90837 — apply to psychotherapy delivered via telehealth.
For telephone-only visits (audio-only telehealth billing), the applicable codes are:
- 99441 — 5 to 10 minutes
- 99442 — 11 to 20 minutes
- 99443 — 21 to 30 minutes
CMS has maintained audio-only telehealth billing for Medicare beneficiaries who cannot access video technology, subject to specific documentation requirements confirming the patient’s inability to use video.
RPM CPT Codes: 99453, 99454, 99457, 99458 Explained
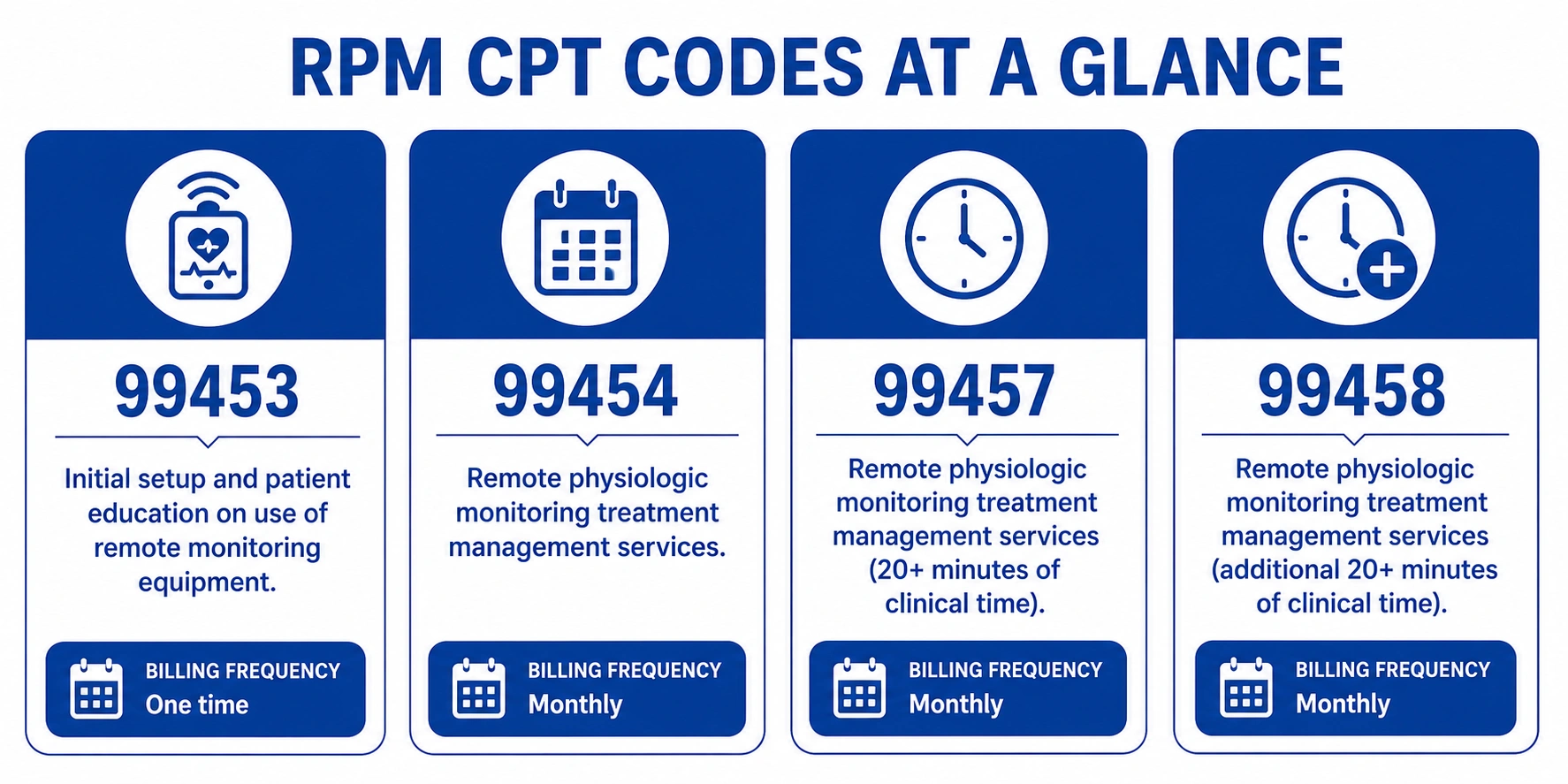
These four RPM CPT codes 2026 form the core of any remote patient monitoring billing program:
| CPT Code | Description | Billing Frequency |
|---|---|---|
| 99453 | Initial patient education and device setup | Once per episode of care |
| 99454 | Device supply and data transmission; 16-day minimum | Monthly |
| 99457 | First 20 minutes of clinical staff interactive communication and review | Monthly |
| 99458 | Additional 20 minutes of clinical staff time (add-on to 99457) | Monthly |
The 16-day minimum monitoring threshold under 99454 is the most frequently missed requirement. Your billing team must confirm that the patient’s device transmitted data on at least 16 separate days within the billing month before this code is submitted.
Remote Therapeutic Monitoring (RTM) CPT Codes: 98975–98981
RTM expands virtual monitoring to non-physiological data and broadens who can bill. Physical therapists, occupational therapists, and speech-language pathologists can now bill RTM codes alongside physicians, making this pathway especially relevant for rehabilitation-focused practices.
Key RTM CPT codes include:
- 98975 — RTM initial device supply, education, and setup
- 98976 — RTM device supply for respiratory monitoring
- 98977 — RTM device supply for musculoskeletal monitoring
- 98980 — First 20 minutes of RTM clinical staff review and interaction
- 98981 — Additional 20 minutes of RTM clinical staff review (add-on)
Audio-Only and Asynchronous Telehealth Billing Codes
Asynchronous telehealth (store-and-forward) refers to services where clinical information is captured and transmitted for review without a real-time interaction. These services use modifier GQ and have more limited Medicare coverage, though several states cover them under Medicaid. Practices offering asynchronous telehealth should confirm state-specific Medicaid policies before embedding these codes into their billing workflow.
The Financial Cost of Telehealth and RPM Billing Errors in 2026
Billing errors in virtual care programs are not minor inconveniences — they represent measurable, recurring revenue loss. Consider these industry benchmarks:
- Telehealth utilization has grown more than 38 times compared to pre-pandemic levels, according to data referenced in AMA telehealth physician adoption surveys, with billing volumes rising proportionally across all specialties.
- The average cost to rework a single denied claim ranges from $25 to over $100, according to MGMA benchmarks — and telehealth claims face denial rates above those of standard in-office visits.
- Medicare Advantage plans cover telehealth differently from traditional Medicare, with some MA plans requiring prior authorization for RPM services that traditional Medicare pays without pre-approval.
- Practices operating RPM programs without structured billing workflows are estimated to collect on fewer than 60% of billable RPM encounters.
- Incorrect modifier use accounts for an estimated 20 to 30% of all telehealth claim denials, according to HFMA revenue cycle benchmarks on virtual care.
These numbers illustrate why telehealth reimbursement accuracy is a direct financial priority — not just a compliance concern.
How Much Revenue Is Your Practice Losing to Telehealth Billing Errors?
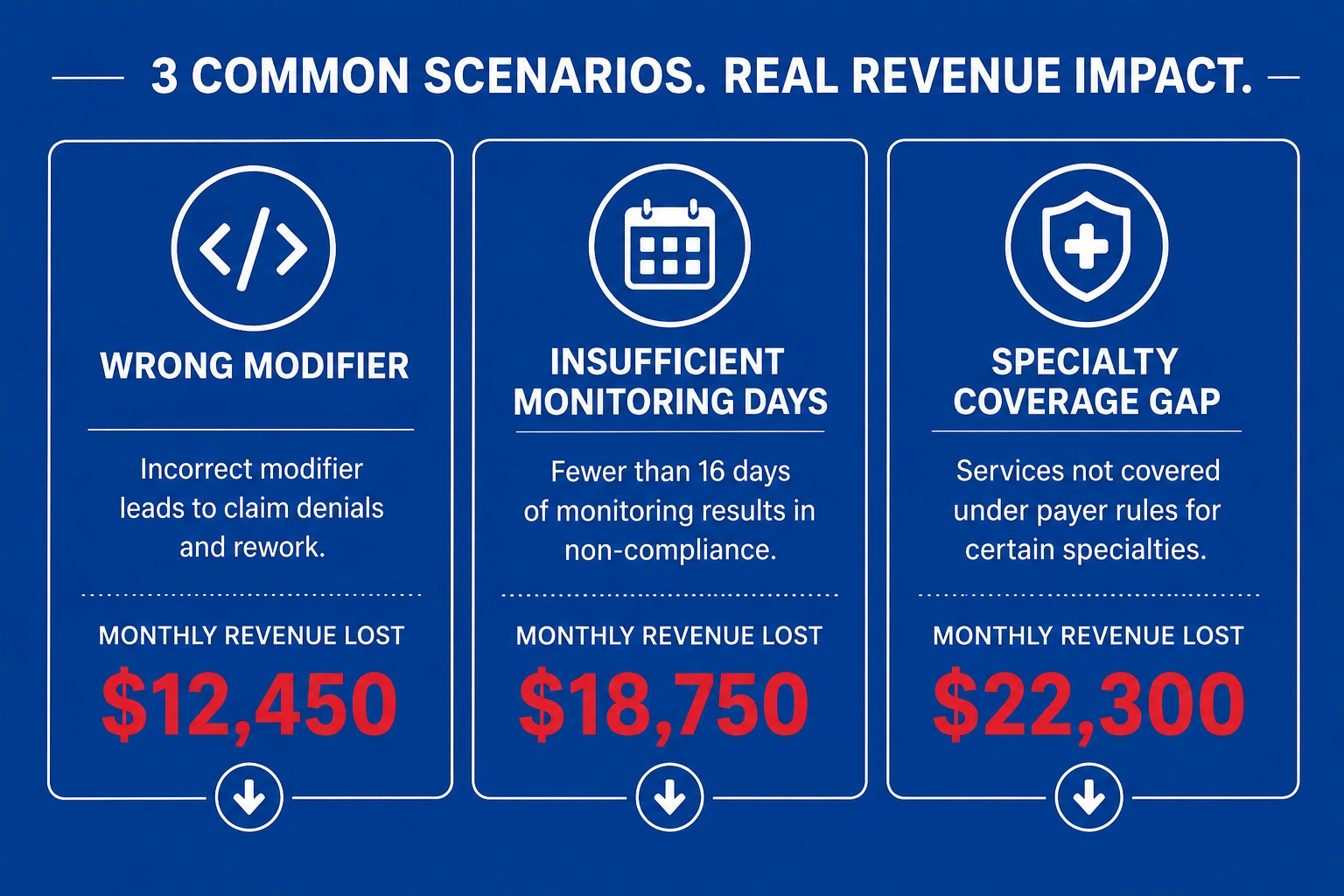
These practice scenarios illustrate the tangible cost of common billing mistakes.
Example 1 — Wrong Modifier Leads to a Blanket Claim Denial
A primary care group bills 200 telehealth visits per month using modifier GT for a commercial payer that requires modifier 95. All 200 claims are denied. At an average reimbursement of $110 per visit, the practice loses $22,000 in a single month — and may face a timely filing deadline before the issue is identified and corrected.
Example 2 — RPM Claims Denied for Insufficient Monitoring Days
A cardiology practice enrolls 50 patients in an RPM program and bills 99454 for all of them at month-end. Post-adjudication, 18 patients failed to transmit data for the required 16 days. Those 18 claims are denied. At approximately $64 per 99454 claim under the 2026 Medicare fee schedule, that is $1,152 in denied revenue — per month, repeating, until the workflow is corrected.
Example 3 — Specialty-Specific Telehealth Reimbursement Gaps
A behavioral health group bills 90837 (60-minute psychotherapy) with POS 02 for a Medicare Advantage patient. The MA plan covers only 90834 (45-minute psychotherapy) for telehealth delivery. The claim is denied. Without a payer-specific coverage review, this billing pattern continues across dozens of patients each month.
Medicare vs. Commercial Payer Telehealth Rules: A 2026 Comparison
What Medicare Covers for Telehealth in 2026
Under CMS telehealth coverage 2026, traditional Medicare covers a broad range of services for beneficiaries regardless of geographic location, including:
- Office and outpatient E/M visits (99202–99215)
- Behavioral health and psychiatric services delivered via video or audio-only
- Chronic care management via telehealth
- RPM services (99453, 99454, 99457, 99458)
- Annual wellness visits
The billing provider must be enrolled in Medicare, and every claim must include the appropriate telehealth modifier and POS code to support payment.
How Commercial Payers Differ From Medicare on Virtual Care
Commercial payer telehealth rules vary widely. Key differences include:
- Prior authorization: Some commercial payers require pre-approval for RPM enrollment
- Covered platforms: Certain plans specify which video technology qualifies for reimbursement
- Reimbursement rates: Commercial rates for telehealth E/M visits range from 80% to 100% of the in-person equivalent depending on plan
- Modifier requirements: Modifier 95 is the commercial standard; GT applies to Medicare
Practices working with a Medical Coding Services partner are better positioned to manage this payer-by-payer variation without increasing their denial rate.
Medicaid Telehealth Coverage Variation by State
Medicaid telehealth rules are state-driven. While all 50 states now cover some form of telehealth under Medicaid, the specific services covered, modifiers required, and audio-only eligibility differ significantly. Practices serving Medicaid patients should maintain a state-specific payer grid that is updated whenever policy bulletins are issued.
Documentation Requirements for Telehealth and RPM Claims
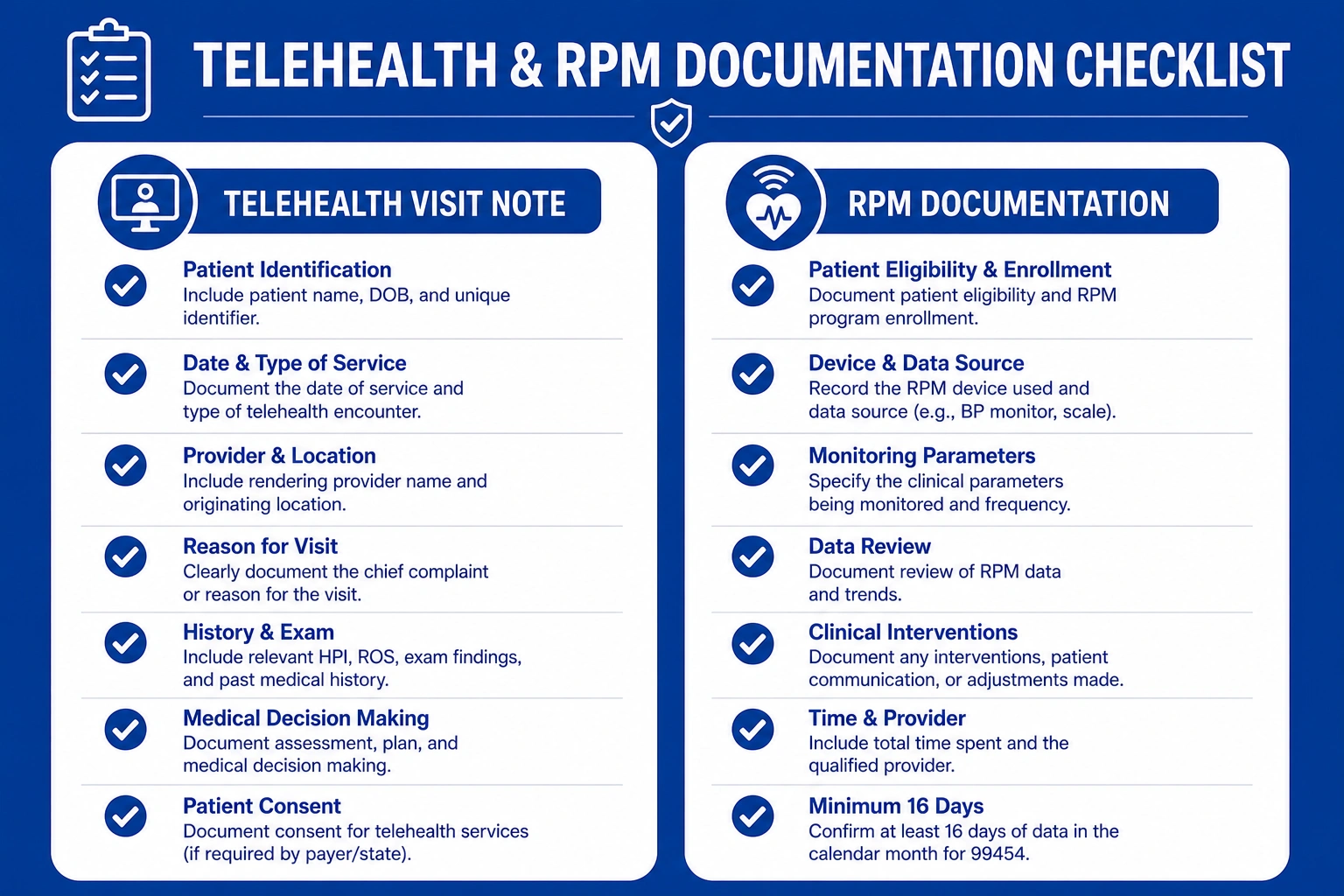
What Must Be in the Telehealth Visit Note
Every telehealth visit note must include:
- Date and time of service
- Patient name and confirmed location at time of visit
- A statement that the service was conducted via telehealth
- Technology platform used, if required by the payer
- Patient consent to the telehealth modality
- Clinical content meeting standard E/M documentation guidelines
RPM Setup, Patient Consent, and Time Documentation Requirements
RPM programs require upfront documentation that many practices overlook at enrollment:
- Written patient consent before RPM begins (required by CMS for Medicare billing)
- Device setup documentation to support 99453 billing
- Monthly data logs confirming at least 16 days of transmission for 99454
- Time-stamped records of clinical staff review for 99457 and 99458
Without this documentation in the patient record, claims are vulnerable to denial on audit even if the clinical service was delivered correctly.
Avoiding Common Documentation Errors That Trigger Audits
The most common documentation errors in telehealth billing compliance include:
- Missing consent documentation in the patient chart
- E/M notes that do not reference the telehealth modality
- Billing 99457 without time-stamped documentation of the clinical review session
- No log of device transmission dates confirming the 16-day RPM threshold
Strategies Every Practice Should Implement Right Now
Use the Correct Place of Service and Modifier Combination
Build a payer-specific reference grid mapping each major payer to the required POS code and modifier combination for telehealth. Review it quarterly and update it whenever a payer issues a coverage bulletin.
Adopt an End-to-End Electronic Workflow for RPM Data
Your RPM platform should automatically capture and log device transmission days, generate monthly data summaries, and flag patients who have not met the 16-day threshold before the billing cycle closes. Manual RPM tracking creates the conditions for systematic billing errors.
Verify Telehealth Coverage Before Every Patient Visit
Eligibility verification for telehealth patients must include a coverage check specific to the virtual service being delivered — not just a general benefits check. This is especially critical for Medicare Advantage and commercial payer patients where telehealth rules diverge from traditional Medicare.
Train Your Billing Staff on Payer-Specific Telehealth Rules
Telehealth billing rules change every year. Your billing team needs structured, recurring training — not a one-time orientation. Develop an internal payer-rule reference document that is updated each plan year and reviewed whenever CMS or a major commercial payer issues a telehealth policy update.
Outsource Telehealth and RPM Billing to Specialists
For practices operating RPM programs at scale, outsourcing to a specialized billing team is often the fastest path to improved collections and lower denial rates. Telehealth billing compliance requires expertise that generalist billing staff may not have — and the cost of errors compounds quickly across a high-volume virtual care program.
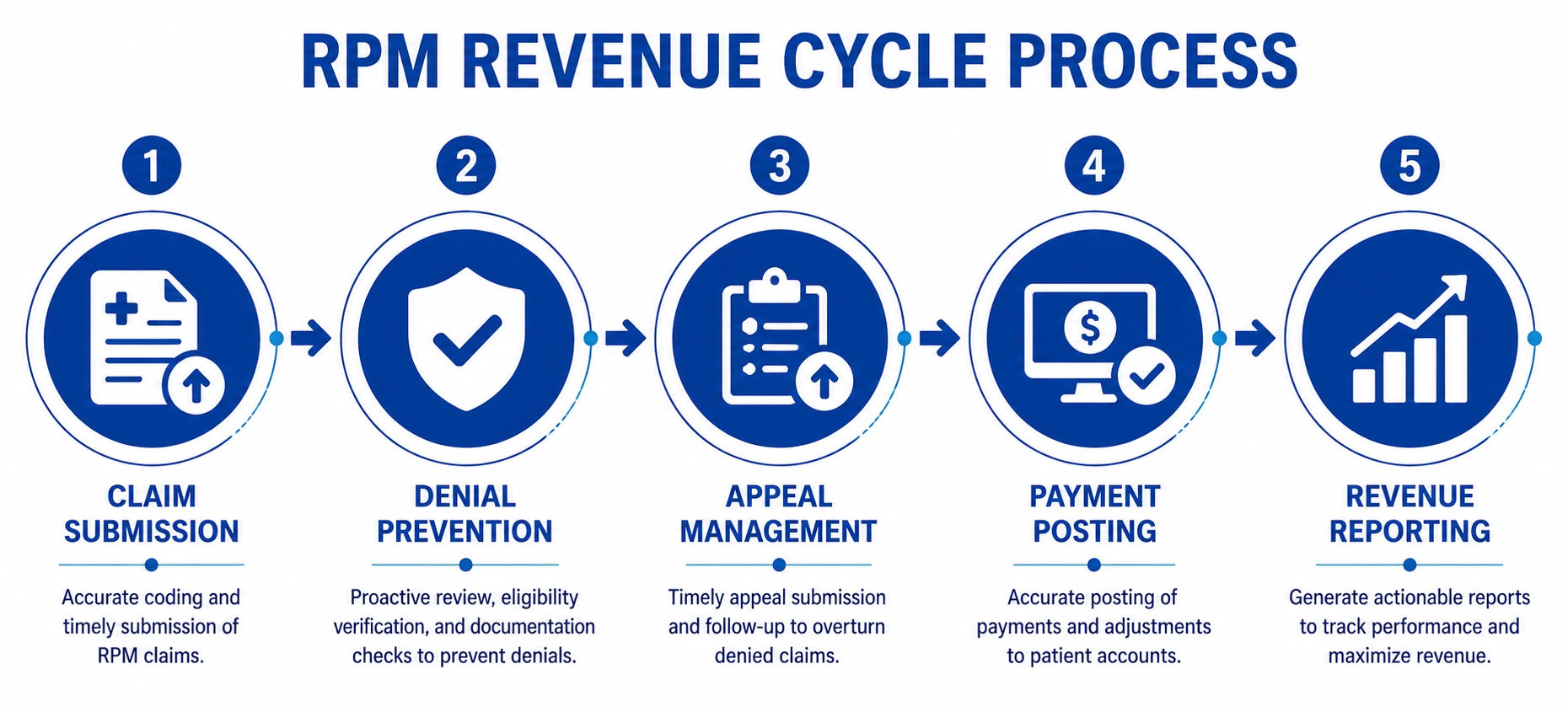
How Outsourced Telehealth and RPM Billing Protects Your Revenue
Proactive Denial Prevention for Virtual Care Claims
A specialized billing team builds payer-specific rules into the claim submission workflow before a single claim goes out the door. This proactive approach catches modifier errors, POS mismatches, and documentation gaps before they reach the payer — reducing denial rates at the source rather than at the appeal stage.
Faster, Fully Documented Appeals
When denials do occur, a specialized team has the telehealth-specific knowledge to build a targeted appeal with the correct supporting documentation. Generic denial management teams often submit incomplete appeals on telehealth claims because they lack familiarity with virtual care billing rules.
Payer-Specific Telehealth Denial Tracking
Outsourced billing teams can maintain granular denial tracking by payer, code, modifier, and denial reason — giving your practice the data it needs to identify systemic billing problems and correct them before they compound into a significant revenue loss.
How TMS Billings Helps Practices Maximize Telehealth and RPM Reimbursement
At TMS Billings, our revenue cycle management team specializes in the unique billing requirements of virtual care programs. We work with primary care practices, specialty groups, and behavioral health providers to:
- Build payer-specific telehealth billing grids that align with each payer’s current modifier and POS requirements
- Implement RPM billing workflows that capture the full 99453–99458 revenue cycle from patient enrollment through monthly claim submission
- Reduce telehealth claim denial rates through front-end eligibility and authorization checks
- Recover revenue from incorrectly denied telehealth and RPM claims through targeted, documentation-supported appeals
- Train your internal staff on payer updates as CMS and commercial payers revise their telehealth policies each year
Whether you are launching your first RPM program or looking to fix a billing workflow generating consistent denials, the TMS Billings team brings the telehealth reimbursement expertise your practice needs in 2026.
Key Takeaways
- Telehealth and RPM billing require payer-specific modifier, POS code, and CPT code combinations — one-size-fits-all billing consistently produces denials
- The four core RPM CPT codes (99453, 99454, 99457, 99458) each carry distinct requirements, especially the 16-day monitoring threshold for 99454
- Medicare Advantage plans apply their own telehealth coverage rules, separate from — and often more restrictive than — traditional Medicare
- Documentation must explicitly support the telehealth modality and, for RPM, include device transmission logs and time-stamped clinical review records
- Proactive denial prevention — not reactive denial management — is the most reliable path to maximizing telehealth reimbursement in 2026
Final Thoughts
Telehealth and RPM billing are among the most complex — and most financially consequential — areas of revenue cycle management in 2026. The rules are detailed, payer variation is significant, and the cost of errors compounds quickly across a high-volume virtual care program.
Your practice does not have to navigate this alone. Whether you need to close a specific billing gap or build an RPM revenue program from the ground up, getting the right support in place now protects your reimbursement for the entire year ahead.