Clinical documentation errors medical coding teams face every single day are more damaging than most practice owners realize. A missing diagnosis, a vague procedure note, or an unsigned order can cascade into a denied claim, a compliance flag, and thousands of dollars in delayed revenue — often without anyone noticing until the damage is done.
For solo practitioners in Brooklyn, group practices in Queens, and multi-specialty clinics across Long Island, the connection between how physicians document and how coders assign codes is direct. When that connection breaks, your revenue cycle pays the price.
If your practice is seeing rising denial rates, frequent coder queries to physicians, or inconsistent reimbursement, documentation problems are almost always at the root. Our Medical Coding Services USA team works with practices across the country that trace most of their coding errors back to one source: incomplete or inaccurate clinical documentation.
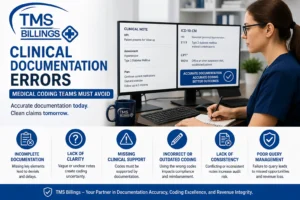
📌 What Are Clinical Documentation Errors in Medical Coding?
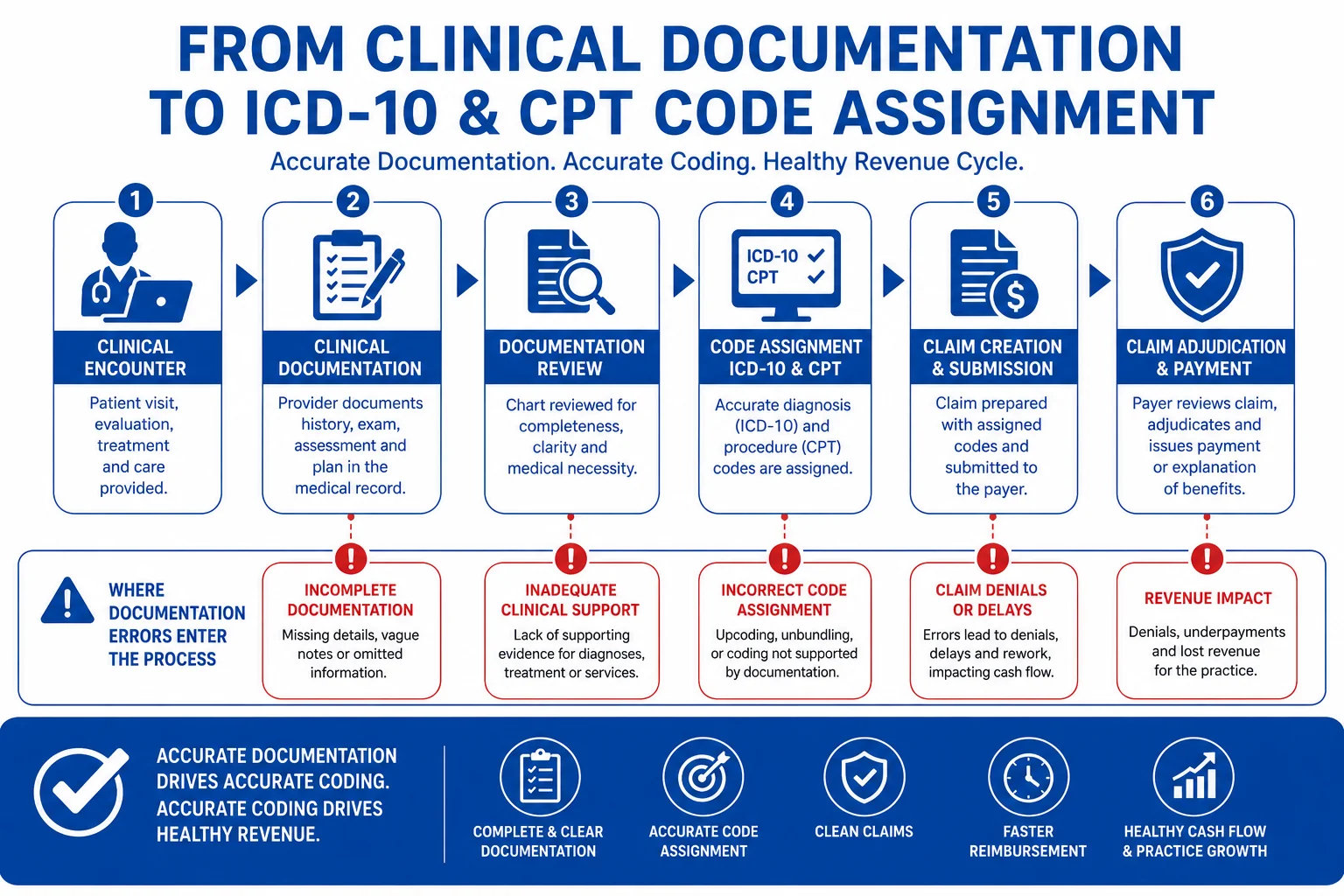
Clinical documentation errors in medical coding occur when physician notes, discharge summaries, or procedure records contain incomplete, vague, or contradictory information that prevents coders from assigning accurate ICD-10, CPT, or HCPCS codes. These errors directly cause claim denials, undercoding, and compliance risks that affect your entire revenue cycle.
Our accurate medical coding services team helps practices close documentation gaps before they become billing problems.
The Real Cost of Clinical Documentation Errors on Medical Coding
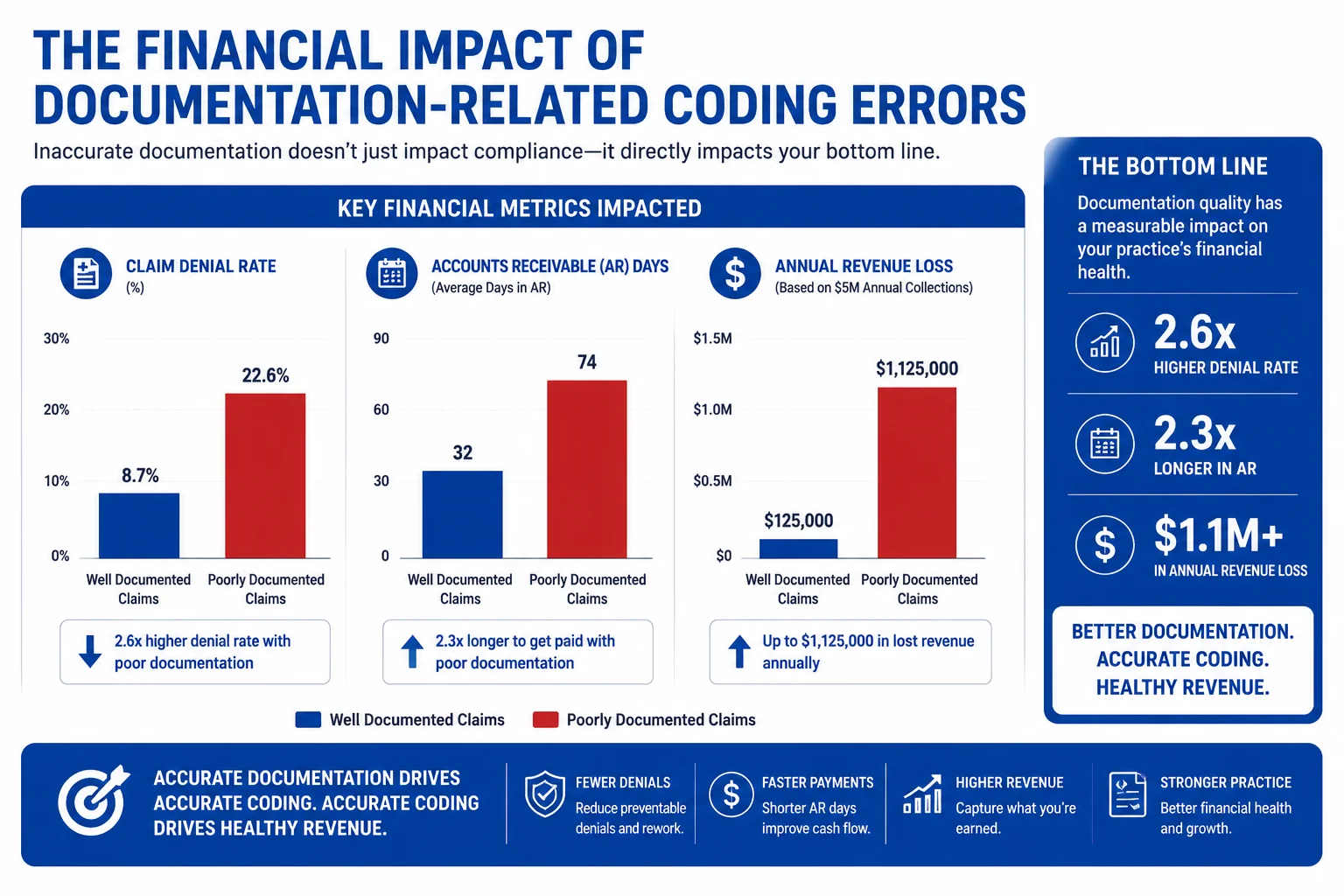
Most practices underestimate how much clinical documentation errors medical coding mistakes actually cost. These are not minor administrative inconveniences. They represent measurable revenue loss, compliance exposure, and operational drag across your entire billing process.
Here is what the data shows:
- Experian Health reports that the US healthcare industry loses over $262 billion annually to claim denials, with documentation errors accounting for a significant share of all preventable denials.
- The American Medical Association reports that one in five claims contains a coding error, many stemming directly from incomplete CPT procedure documentation and unsupported evaluation and management levels.
- MGMA benchmarking data shows practices without a CDI program carry average AR days of 40–50, compared to 30–35 for those with structured clinical documentation improvement protocols in place.
- The Office of Inspector General has identified clinical documentation deficiencies as one of the top causes of improper Medicare payments, with error rates reaching double digits in high-risk specialties.
- AAPC research shows that practices with certified coders working from complete documentation achieve clean claim rates above 95%, while those without CDI support average as low as 75–80%.
- Per CMS ICD-10 guidelines, codes must be supported by physician documentation in the medical record. When documentation is vague, coders default to unspecified codes — which reimburse at lower rates and often trigger payer audits.
- AHIMA estimates that reworking a single denied claim due to a coding error costs between $25 and $118 in administrative labor alone, not counting the revenue delay.
- HHS and HIPAA compliance standards require that medical records accurately reflect the services provided — meaning documentation gaps create not just coding errors but direct legal exposure.
Practices that outsource their coding to AAPC-certified medical coders consistently outperform those relying on internal teams without documentation support.
📣 Is Your Practice Losing Revenue to Documentation Errors?
Is your denial rate climbing? Are your coders spending more time chasing physicians for clarification than actually coding?
The TMS Billings team offers a free coding review that pinpoints exactly where your documentation is creating coding errors and revenue loss. Speak with our medical coding services team today — before documentation problems cost your practice another full billing cycle.
Common Clinical Documentation Errors That Lead to Medical Coding Mistakes

Understanding what causes the problem is the first step to fixing it. Medical coding errors from poor documentation tend to cluster around the same failure points across specialties and practice sizes.
| Error type | ❌ Vague documentation | ✓ Specific documentation | Coding consequence |
|---|---|---|---|
| Non-specific diagnosis | “Worsening heart condition” | “Ischemic heart disease with diastolic heart failure” | Forces unspecified ICD-10 code; lower reimbursement and payer audit risk |
| Missing laterality | “Knee pain” | “Left knee pain, lateral compartment” | Blocks specific ICD-10 assignment in orthopedics; claim delayed or denied |
| Missing or unsigned order | Verbal order, no written follow-through | Signed written order with date and clinical indication | Coder cannot assign CPT code; claim blocked from submission |
| Unsupported E/M level | Level 4 billed; note reflects brief assessment only | MDM or total time documented to support selected E/M level | Compliance risk; downcode required or practice faces audit exposure |
| Missing comorbidities | “HTN in problem list, not addressed in note” | “Hypertension, managed — BP reviewed today” | HCC condition goes uncoded; RAF score reduced for Medicare Advantage patients |
| Incomplete operative note | “Procedure performed without complication” | Approach, laterality, findings, and complications documented | Undercoding, incorrect modifier use, and rejected surgical claims |
| Unspecified psych diagnosis | “Anxiety” | “Generalized anxiety disorder, moderate severity” | DSM-aligned ICD-10 code blocked; unspecified code reimburses at a lower rate |
Vague or Non-Specific Diagnosis Language
ICD-10 coding documentation errors most often begin with physician notes that use general, non-specific language. Phrases like “patient has chest pain” without clinical context force coders to assign unspecified ICD-10 codes — limiting reimbursement and triggering payer scrutiny.
A cardiologist in Manhattan, for example, may document “worsening heart condition” in a note that should specify ischemic heart disease, diastolic heart failure, or an arrhythmia. Each diagnosis carries a different ICD-10 code and a different reimbursement value. Vague documentation costs that practice money on every single claim.
Missing or Unsigned Orders
Coders cannot assign CPT codes for procedures without documented physician orders. Missing signatures, late-signed orders, and verbal orders with no written follow-through create gaps that block accurate code assignment. This is one of the most common incomplete documentation coding mistakes in outpatient and ambulatory settings.
Unsupported Evaluation and Management Levels
E/M coding requires documentation that supports the selected level of service. When a physician bills a Level 4 or Level 5 visit but the note reflects only a brief assessment, coders face a compliance problem — and the practice faces audit risk. AMA’s updated E/M guidelines require that medical decision-making or total time documentation be clear and complete.
Missing Comorbidities and Secondary Diagnoses
HCC risk adjustment documentation depends on capturing all chronic conditions that influence patient care. When coders cannot see documented comorbidities — diabetes, hypertension, CKD — those conditions go uncoded, reducing your RAF scores and HCC accuracy. This is an especially costly documentation gap for practices serving Medicare Advantage patients across the Bronx and Long Island.
Operative Note Gaps
For surgical and procedural specialties, the operative note must clearly state what was performed, the approach used, and any findings or complications. Incomplete operative notes lead to undercoding, incorrect modifier use, and rejected claims. ICD-10 CPT HCPCS code accuracy depends entirely on what is — and what is not — written in that record.
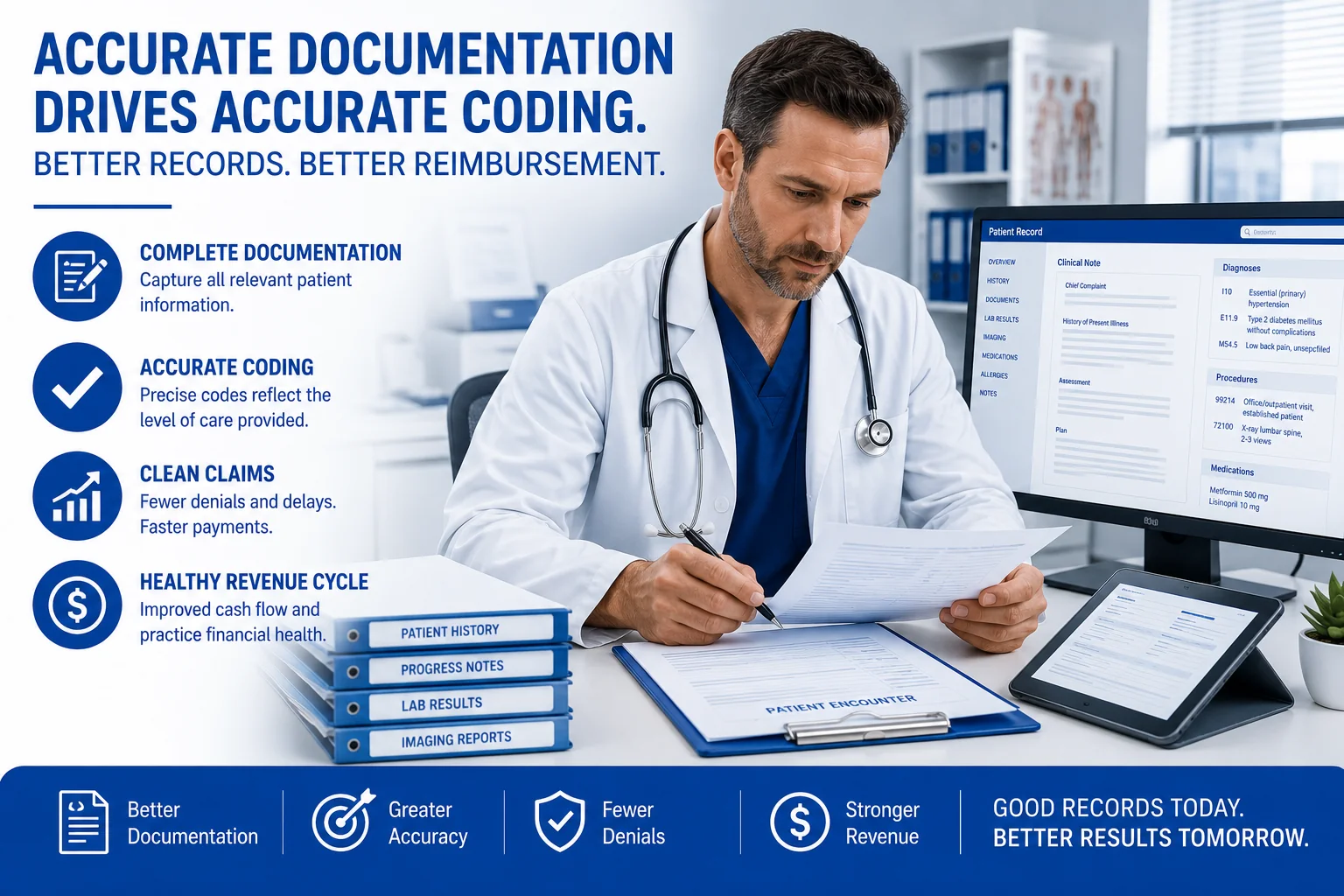
How Clinical Documentation Errors Affect ICD-10 and CPT Coding Accuracy
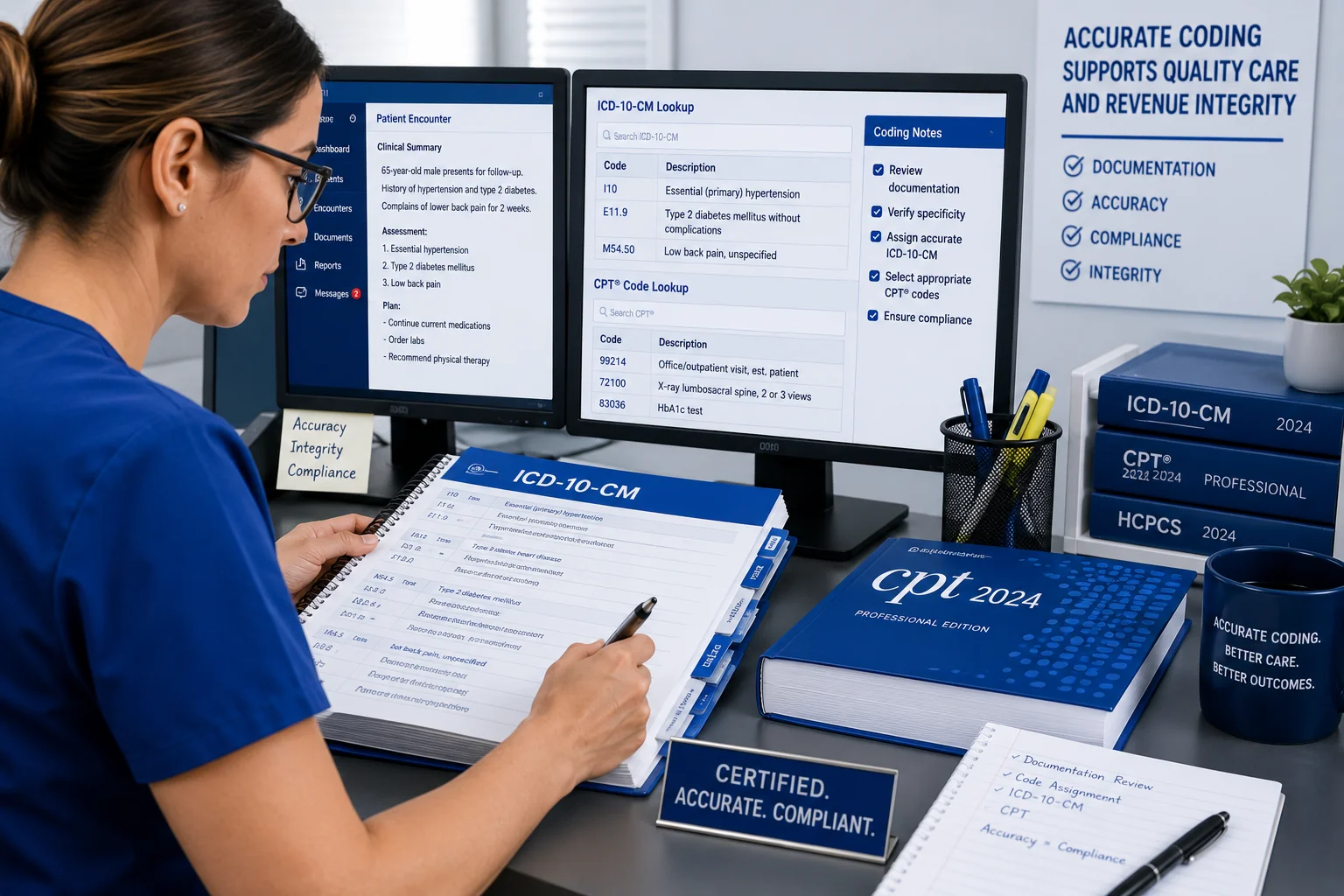
Medical coding accuracy documentation is not just a billing issue. It is a clinical integrity issue. Coders are trained to code what is documented — not what they infer or assume. This is both an AAPC standard and a CMS requirement.
Clinical Documentation Errors Medical Coding Teams Cannot Work Around
When a physician at a Queens internal medicine practice documents “patient with elevated blood sugar” instead of “Type 2 diabetes mellitus, uncontrolled,” the coder cannot assign the correct ICD-10 code — even if the intent is obvious. The result is either an unspecified code that underpays, or a query back to the physician that delays the claim by days.
This pattern repeats across every specialty:
- In orthopedics, “knee pain” without laterality blocks specific ICD-10 assignment
- In psychiatry, “anxiety” without a specified subtype prevents accurate DSM-aligned coding
- In primary care, “fatigue” without an established cause can block coding of the underlying chronic condition
Clinical documentation improvement medical coding programs address these gaps before claims are submitted — not after denials arrive.
Does Your Practice Have a Clinical Documentation Problem? A Quick Checklist
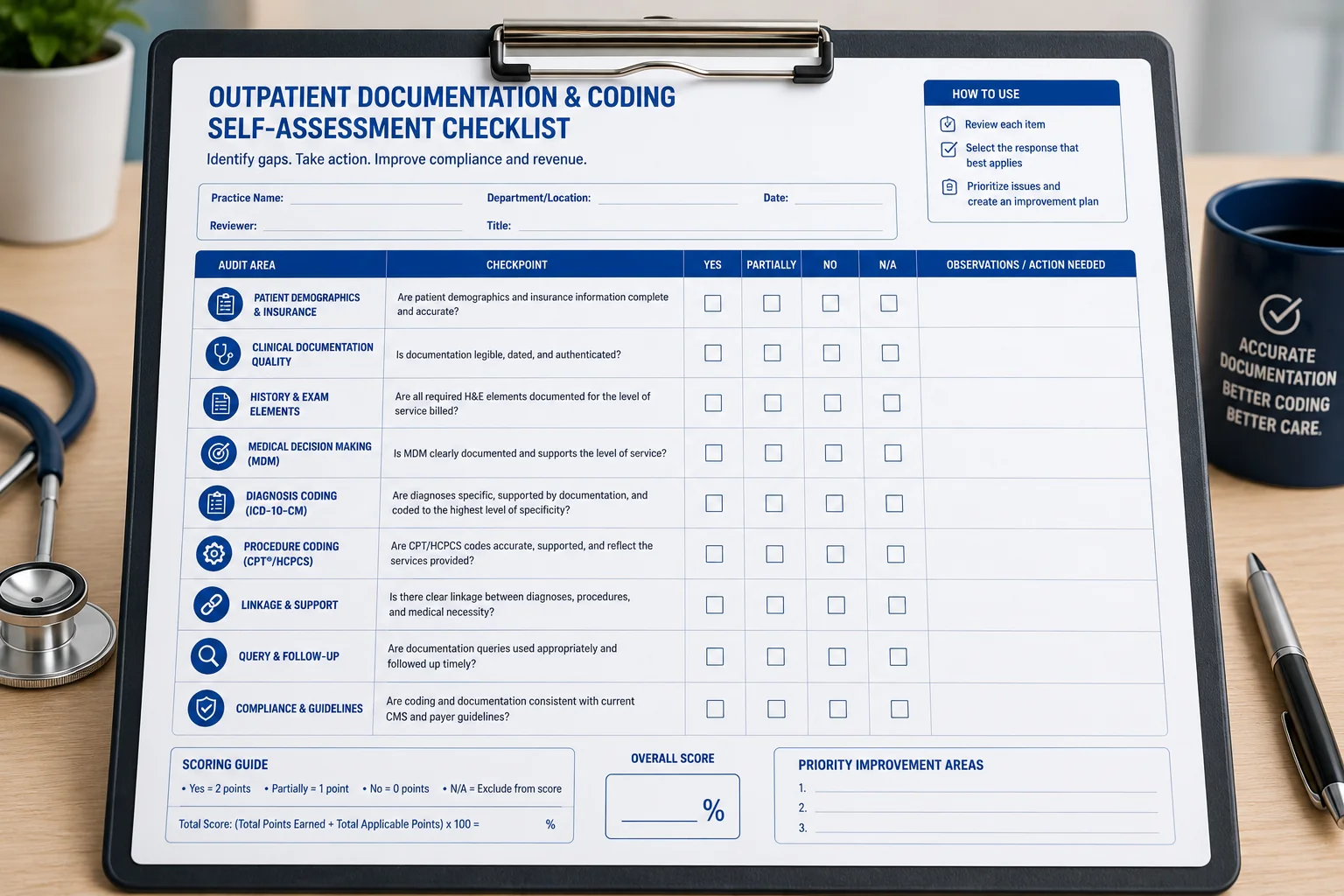
Run through this list. If your practice checks more than three or four of these boxes, documentation errors are actively affecting your coding accuracy and revenue.
- Your coders frequently query physicians for missing diagnosis details
- Your claim denial rate is above 5% with coding errors as the primary cause
- ICD-10 codes are being assigned based on inference, not documented specifics
- Your practice has no formal CDI clinical documentation improvement program
- Discharge summaries are incomplete, late, or missing key clinical details
- Documentation uses vague language like “pain,” “infection,” or “disorder” without specificity
- Coding audits reveal recurring errors in the same diagnosis or procedure code categories
- Physicians are unaware of how their documentation directly affects coding accuracy
- Your AR days are above the MGMA benchmark for your specialty
- Operative notes frequently omit approach, laterality, or complication details
- Modifiers are applied inconsistently due to unclear procedure documentation
- Chronic conditions appear in the problem list but are not addressed in the visit note
- E/M levels are not supported by the documented medical decision-making
- Your clean claim rate has dropped below 90%
- Your coders are defaulting to unspecified codes more than 15% of the time
If several of these apply, it is time to take action. Clinical documentation improvement and coding support from a dedicated team can reduce these errors significantly within 30 to 60 days.
What Is CDI and How Does It Reduce Medical Coding Errors?

Clinical documentation improvement (CDI) is a structured program that closes the gap between clinical care and medical coding. CDI specialists review documentation in real time or retrospectively, identify gaps and ambiguities, and work with clinical staff to ensure the medical record accurately reflects what happened and what was treated.
In practice, a CDI program does several important things:
- Reduces physician query rates by proactively educating clinical staff on documentation standards
- Improves ICD-10 and CPT code accuracy by giving coders complete, specific information
- Supports HCC risk adjustment documentation for Medicare Advantage populations
- Reduces the accounts receivable impact coding errors create by catching problems before submission
- Drives clean claim rate improvement across the full revenue cycle
- Supports HIPAA coding compliance and protects your practice during payer audits
A pediatric group practice in the Bronx that implemented a CDI program with a certified team saw their denial rate drop from 12% to under 4% within two quarters. Physicians required fewer follow-up queries, claims moved faster, and reimbursement improved across the board.
AHIMA sets the national standards for CDI programs, and practices that align with those standards consistently outperform those without them.
Our certified medical coding team integrates CDI principles into every coding review — ensuring your documentation supports accurate claims the first time.
How Documentation Errors Impact Revenue Cycle Management
Poor documentation does not just cause denials. It creates compounding downstream effects across your entire revenue cycle management documentation process.
When a claim is denied due to a coding error rooted in missing documentation, here is what actually happens:
- The claim enters accounts receivable and often sits for 30 to 90 days
- Staff must pull the record, identify the error, correct the code, and resubmit
- If the documentation cannot support a corrected code, the claim may be written off entirely
- The physician must be contacted for an amendment or addendum — adding clinical time to the cost
- Payers may flag the practice for a billing audit if denials form a recognizable pattern
This cycle — deny, rework, resubmit, delay — is what drives AR days up and net collection rates down. Practices without CDI programs absorb these inefficiencies silently, often mistaking them for normal billing friction.
Healthcare revenue recovery after a denial is always more expensive than prevention. Insurance claim denial documentation patterns also invite OIG scrutiny when coding errors are systematic and unaddressed. The cost of an audit far exceeds the cost of a documentation fix.
What Your Practice Should Do Right Now
If your practice is experiencing high denial rates, slow AR days, or frequent coder-to-physician queries, the fix starts with documentation — not just coding. Here are five concrete steps to get there.
1. Run a coding audit. Identify which codes are being denied most frequently and trace each denial back to the documentation that supported it. You will quickly see the patterns.
2. Educate your clinical staff. Physicians and nurses should understand how their language directly affects code assignment and reimbursement. A short documentation training session can shift outcomes immediately.
3. Implement a CDI process. Even a basic pre-submission documentation review can dramatically improve coding accuracy and reduce how poor clinical documentation causes medical coding errors at your practice.
4. Partner with certified coders. AAPC-certified medical coders who understand both documentation standards and payer requirements reduce error rates and improve first-pass resolution across the board.
5. Track and benchmark. Use clean claim rate, denial rate by code category, and AR days as your leading indicators. Compare against MGMA benchmarks for your specialty every quarter.
Your practice does not have to absorb the cost of documentation-related coding errors. Professional medical coding services USA give your practice the expertise to stop the cycle and get claims right the first time.
Conclusion
Clinical documentation errors medical coding teams encounter every day are preventable — but only when your practice has the right systems, training, and partners in place. From vague diagnosis language to missing procedure details, documentation gaps cost practices real money and create real compliance exposure across every billing cycle.
The solution is not just to code better. It is to document better — and to work with a team that understands how to close the gap between clinical care and accurate claims. Our expert medical coding services team is ready to help your practice stop losing revenue to documentation errors and start building a revenue cycle that actually works.
Reach out to TMS Billings today to schedule your free coding review.