How AI-Driven Prior Authorization Denials Are Costing Practices in 2026 (and How to Fight Back)
If your practice has felt a sharp uptick in denied claims this year, you are not imagining it. Prior authorization denials 2026 trends show payers leaning harder on artificial intelligence to review, flag, and reject requests faster than ever — often before a human reviewer ever looks at the case. For physicians, practice managers, and billing teams already stretched thin, this shift is quietly draining revenue that used to come through without a fight.
At TMS Billings, our Revenue Cycle Management Services team works inside payer portals every day, and we are seeing the same pattern across specialties: approvals that once took 48 hours now bounce back instantly denied, with appeal windows shrinking before anyone notices. Practices that pair strong documentation with a regular Medical Billing Audit Services review are catching these denials early — before they become unrecoverable revenue.
What Are AI-Driven Prior Authorization Denials?
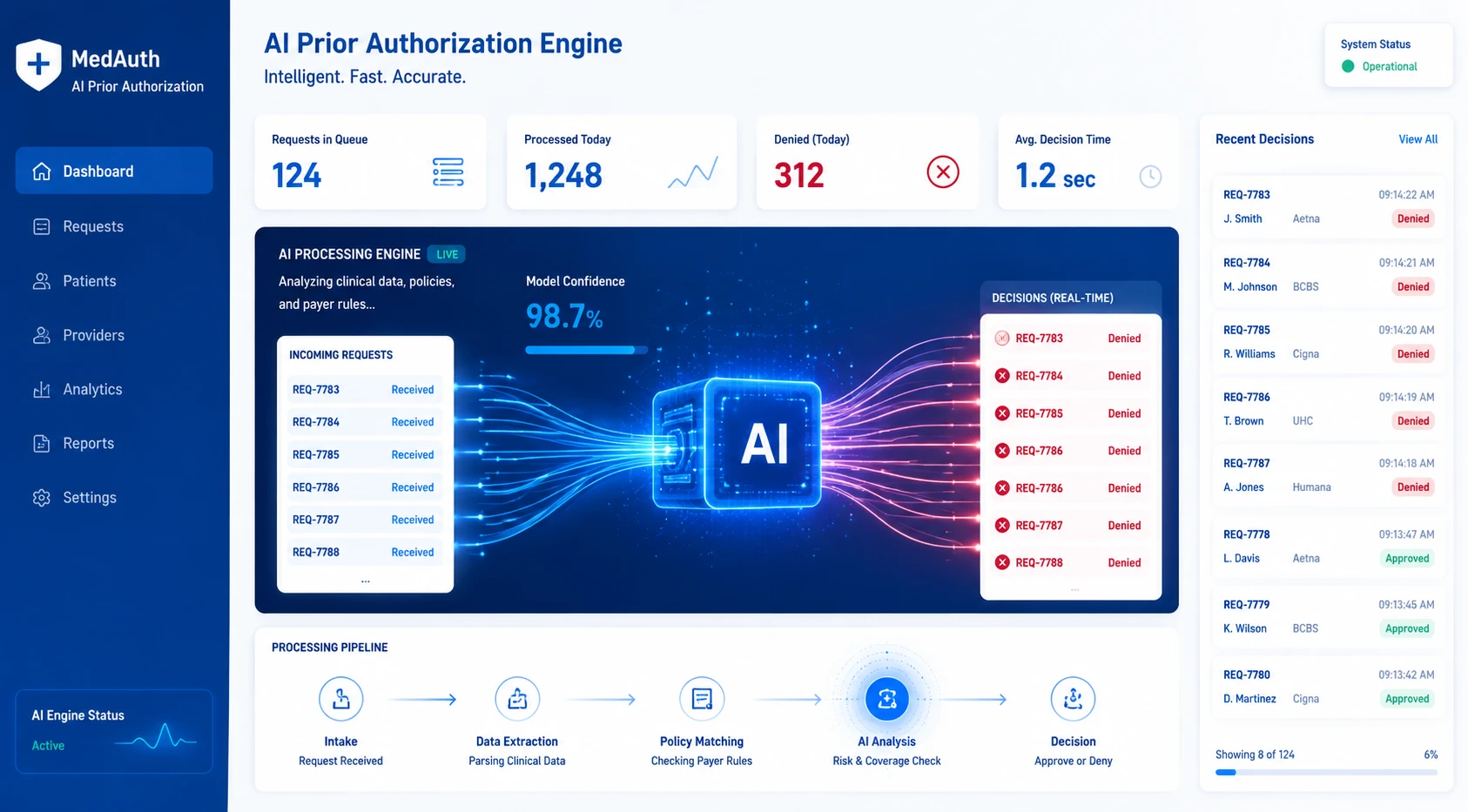
AI-driven prior authorization denials happen when a payer’s algorithm — rather than a human reviewer — automatically rejects a request based on coded criteria or pattern-matching against past claims. These denials can occur within seconds of submission, often flagging cases a human reviewer would approve, and they are a major driver of prior authorization denials in 2026.
Why AI Prior Authorization Denials Are Rising Faster Than Ever in 2026
Physician concern is no longer anecdotal. In a recent AMA physician survey, 61% of physicians said they believe payers’ unregulated use of AI is increasing prior authorization denials, and three-quarters reported that denial volume has climbed over the past five years. Nearly one in three said their prior auth requests are now often or always denied. For a billing team, that translates directly into more reworked claims, more appeals, and more staff hours spent chasing approvals that used to clear on the first pass.
The Difference Between Traditional Denials and AI-Driven Prior Authorization Denials in 2026
Traditional denials usually trace back to a specific, identifiable error — a missing modifier, an expired authorization, a coding mismatch. AI-driven denials behave differently. They’re issued by algorithms trained to flag statistical outliers, which means a clean, well-documented request can still be denied if it doesn’t match the payer’s model of a “typical” approved case. That makes prior authorization denials 2026 harder to predict and harder to prevent using last year’s playbook.
Why Many Practices Don’t Notice the Revenue Impact Right Away
AI-driven denials often arrive fast and look routine, so they get batched into the same follow-up queue as everyday denials. Without specialty-specific tracking, a practice can lose tens of thousands of dollars over several months before anyone connects the dots. By the time the pattern shows up in an aging report, several appeal deadlines have likely already passed.
The Hidden Cost of Shrinking Appeal Windows
Many payers have quietly tightened appeal windows as their internal review processes have automated. A request that once allowed 60 days to appeal might now allow 30, and a denial issued instantly by an algorithm still carries the same clock. Practices relying on manual tracking — spreadsheets, sticky notes, shared inboxes — are the most likely to miss these compressed deadlines and write off revenue that was actually recoverable.
The Biggest Drivers Behind AI Prior Authorization Denials
Several forces are converging at once, and most practices are dealing with more than one of these at the same time.
Automated Payer Review Systems
Large payers, including several Medicare Advantage plans, now route a significant share of prior auth requests through automated review before any human sees the file. These systems are built for speed and consistency, not nuance, and they tend to deny anything outside a narrow, pre-coded pattern — even when the clinical justification is sound.
Inconsistent Gold Carding Enforcement
Prior authorization gold carding is supposed to exempt high-performing providers from routine review, but enforcement remains uneven. Texas providers can qualify with a 90% approval rate over a defined lookback period, and UnitedHealthcare’s national gold card program sets the bar at 92% approval over a two-year window — yet only a small share of providers nationally have actually been confirmed eligible. Until prior authorization gold carding is enforced consistently across payers and states, most practices will keep facing the same review volume regardless of their track record.
Documentation Gaps That Trigger Auto-Denials
AI review tools are unforgiving about incomplete data fields, missing clinical notes, or codes that don’t align cleanly with the requested service. A documentation gap a human reviewer might have called the office to clarify will often trigger an automatic denial instead, with no chance to fix it before the rejection is issued.
Medicare Advantage Plan Complexity
Medicare Advantage prior auth denials carry their own complexity, since each plan applies its own coverage criteria on top of CMS rules. With the vast majority of Medicare Advantage enrollees in plans that require prior authorization for at least some services, small differences in plan-specific criteria can produce inconsistent outcomes for the same diagnosis and treatment plan across different patients.
New CPT Codes Outpacing Payer Rules
New and revised CPT codes are released faster than payer systems can update their automated review criteria. When a code doesn’t match an existing rule in the payer’s algorithm, the safest default for that system is often a denial, leaving practices to untangle a coding mismatch that has nothing to do with medical necessity.
Staffing Gaps in Prior Auth Follow-Up
Many practices haven’t scaled their prior auth staff to match the new volume of automated reviews and appeals. A meaningful share of physician practices already employ staff dedicated solely to prior authorization, and without similar investment elsewhere, follow-up tasks slip, deadlines pass, and recoverable revenue quietly disappears.
How Much AI Prior Authorization Denials Are Costing Practices in 2026
Industry benchmarks make the scale of the problem clear. MGMA and HFMA data put the typical industry denial rate between 6% and 13%, with more than half of healthcare organizations now reporting rates above 10% — well past the roughly 8% MGMA considers a healthy ceiling. Separate MGMA polling found 41% of providers reporting denial rates above 10%, a trend that has continued into 2026. These claim denial trends compound quickly: HFMA and MGMA estimate the cost to rework a single denied claim at $25 to $118, and a practice processing hundreds of denials a month can lose tens of thousands of dollars annually in rework alone, before counting lost or delayed reimbursement.
Medicare Advantage prior auth denials illustrate the payer-specific gap. Across Medicare Advantage plans, more than 50 million prior authorization requests were submitted in a recent year, and roughly 3.2 million were partially or fully denied. Only about 11.7% of those denials were appealed — yet when practices did appeal, more than 80% were overturned. That gap between what gets denied and what actually gets challenged is where most uncollected revenue is hiding.
Gold carding was designed to close this gap, but the rule and the reality haven’t caught up with each other. Even in Texas, where the gold card law has existed since 2021, only a small percentage of providers qualified for an exemption in the program’s first year. A practice that works hard to reduce prior authorization denials may still face the same review volume as a lower-performing colleague until enforcement catches up. For full regulatory context, see the CMS Interoperability and Prior Authorization Final Rule, which requires payers to begin publicly reporting approval, denial, and turnaround metrics in 2026.

Example 1 — Missed Appeal Windows
Consider a five-physician orthopedic group that didn’t realize one of its top payers had shortened its appeal window from 60 to 30 days. By the time staff caught the pattern, more than a dozen denials had passed the deadline, representing nearly $40,000 in unrecoverable claims for a single quarter.
Example 2 — High-Approval Physicians Still Getting Denied
A cardiology practice with a historical 95% prior auth approval rate began seeing automated denials on nearly identical requests it had submitted successfully for years. Nothing in its documentation process had changed — the payer’s AI model had simply shifted its criteria, and the practice had no easy way to know until denials started piling up.
Example 3 — Specialty-Specific Denial Spikes
Endocrinology and other specialties tied to high-cost specialty drugs have seen some of the sharpest denial spikes, since these requests are prime targets for automated review. A practice that tracks its own denial trends closely can catch a spike within weeks instead of discovering it in a quarterly financial review.
Not sure how much revenue your practice is losing to prior authorization denials? A focused prior authorization and denial audit can show you exactly where requests are stalling, which payers are denying the most, and how much is realistically recoverable. Our team can assess your current revenue cycle exposure and outline a plan to reduce prior authorization denials before they erode another quarter of revenue.
How to Identify AI-Driven Denial Patterns in Your Practice
Key Warning Signs
- Denials arriving with little or no explanation beyond a generic code
- Approval rates dropping for services that were previously routine
- Denials issued within minutes of submission
- One payer’s denial rate climbing while others stay flat
- Repeated denials for the same CPT code across multiple patients
- A high success rate when staff do challenge a denial through appeal
Revenue Cycle Metrics to Monitor
- First-pass approval rate by payer
- Denial rate by CPT code and specialty
- Average prior authorization turnaround time
- Percentage of denials appealed versus written off
- Appeal win rate
Conducting a Prior Authorization Audit
A focused audit pulls your last 90 days of prior auth submissions and sorts them by payer, outcome, and turnaround time. Look specifically for clusters of denials tied to one payer or one code — that pattern usually points to an automated review rule rather than a documentation problem on your end. This kind of review is also one of the fastest ways to surface AI-driven denial patterns before they show up in your aging report.

Strategies to Fight Back Against AI Prior Authorization Denials
The good news: most of what drives AI-related denials can be addressed with consistent process changes.
Strengthen Documentation Before Submission
AI review tools deny incomplete files instantly, so completeness matters more than ever. Build a standardized intake template for each frequently-requested service that captures every data point the payer’s system checks, and train staff to flag missing fields before submission rather than after a denial arrives.
Use Real-Time Eligibility and Electronic Prior Auth (ePA)
Electronic prior authorization (ePA) tools that check eligibility and submission requirements in real time catch errors before they reach the payer’s automated review, cutting down on the documentation gaps that drive instant denials. Practices using ePA consistently report faster turnaround and fewer denials tied to missing information.
Track Appeal Deadlines Aggressively
Build a denial management software workflow — even a simple shared tracker — that flags appeal deadlines the moment a denial is logged, not when staff get around to reviewing it. Given how often appealed denials are overturned, a missed deadline is often the single most expensive mistake in the entire prior auth appeal process.
Monitor Gold Carding Eligibility by State
Prior authorization gold carding rules vary significantly by state and by payer, and eligibility windows can open and close without much notice. Track your approval rate by payer year-round so you’re ready to apply the moment your practice qualifies, rather than discovering months later that you missed an exemption window.
Invest in Dedicated Prior Authorization Staff
Whether through hiring or outsourcing, a dedicated point person for prior authorization denial management prevents requests from falling into a generic billing queue where deadlines slip. Practices with a clear owner for this function consistently catch AI-driven denial patterns faster than those treating prior auth as a shared, ad hoc task.
Prior Authorization Denial Prevention Checklist
- Verify eligibility and benefits before scheduling any service requiring prior auth
- Use a payer-specific documentation template for high-volume CPT codes
- Confirm prior auth approval status before the date of service, not after
- Flag missing clinical notes or test results before submission
- Submit through electronic prior authorization (ePA) whenever the payer supports it
- Log every denial with payer, CPT code, reason, and date received
- Set an automatic reminder at submission for the applicable appeal deadline
- Review denial reason codes weekly for repeat patterns by payer
- Track first-pass approval rate by payer on a monthly basis
- Confirm your practice’s current gold carding eligibility status with each major payer
- Escalate denials tied to identical, previously-approved requests for manual payer review
- Train front-desk and clinical staff on payer-specific submission requirements
- Audit a sample of denied claims quarterly to identify root cause
- Maintain a denial management software or tracking system staff actually use
- Reassess outsourcing prior authorization workflows if in-house follow-up consistently falls behind

How Outsourced Prior Authorization & Denial Management Helps Recover Revenue
Proactive Denial Prevention
An experienced outsourced team reviews documentation against payer-specific criteria before submission, catching the gaps that trigger automated denials. This proactive denial prevention approach catches issues at the front end, where they’re cheapest and fastest to fix, instead of after a denial has already cost the practice time and revenue.
Faster, Better-Documented Appeals
When a denial does happen, a dedicated team can move quickly through the prior auth appeal process with payer-specific documentation already on hand, instead of starting from scratch. Given how often appeals succeed once filed, speed and completeness in that appeal package directly protect recoverable revenue.
Payer-Specific Denial Tracking
Outsourced denial management teams typically track denial patterns across every payer a practice works with, spotting a new automated review rule or a shrinking appeal window faster than an in-house team juggling multiple responsibilities. That visibility is often what separates a practice that adapts quickly from one that loses months of revenue before noticing a problem.
How TMS Billings Helps Practices Fight AI Prior Authorization Denials
At TMS Billings, our revenue cycle automation tools and dedicated prior authorization specialists work payer by payer, tracking turnaround times, denial reasons, and appeal outcomes so your billing team isn’t flying blind. We build payer-specific submission checklists for your highest-volume services, monitor your practice’s gold carding eligibility as approval rates shift, and manage the prior auth appeal process from the moment a denial lands — not after the deadline has passed.
Our team also runs ongoing revenue cycle reviews to catch denial patterns before they compound, layering in coding and documentation audits for specialties seeing the sharpest spikes, including orthopedics and endocrinology. The goal is straightforward: fewer denials, faster appeals, and a clear, payer-specific view of where your revenue is actually at risk in 2026.

Key Takeaways
- AI-driven prior authorization denials are issued faster and are harder to predict than traditional denials.
- Appeal windows are shrinking industry-wide, making fast tracking essential.
- Gold carding exists but isn’t consistently enforced, so most practices still face full review volume.
- Medicare Advantage prior auth denials affect millions of requests annually, with a high overturn rate on appeal.
- The cost to rework a single denied claim ranges from $25 to $118, compounding quickly at scale.
- A focused prior authorization denial management strategy — in-house or outsourced — is the most reliable way to reduce prior authorization denials and protect revenue in 2026.
Final Thoughts
Prior authorization denials in 2026 are not a temporary spike — they reflect a structural shift in how payers review claims, and that shift isn’t reversing. Practices that wait for gold carding enforcement to catch up, or assume their historically strong approval rate will protect them, are likely to keep losing recoverable revenue to denials they never even notice.
The practices holding steady are the ones treating prior authorization denial management as an ongoing, measured process: tracking metrics by payer, tightening documentation before submission, and moving fast on appeals. That shift in approach, more than any single tactic, is what separates practices protecting their revenue from those quietly absorbing the loss.