

Modifier 25 vs Modifier 59: When to Use Each
If your coders can’t explain the modifier 25 vs modifier 59 decision in one sentence, your claims are probably paying the price for it. These two modifiers get confused constantly, and that confusion drives real revenue loss: bundled E/M visits, denied procedure lines, and payer audits that dig years into the past. Getting the modifier 25 vs modifier 59 distinction right, every time, is one of the fastest ways to protect your clean claim rate and keep your denial rate down. Whether you run coding in-house or lean on outsourced medical billing services, your coders and your denial rate depend on getting this right the first time.
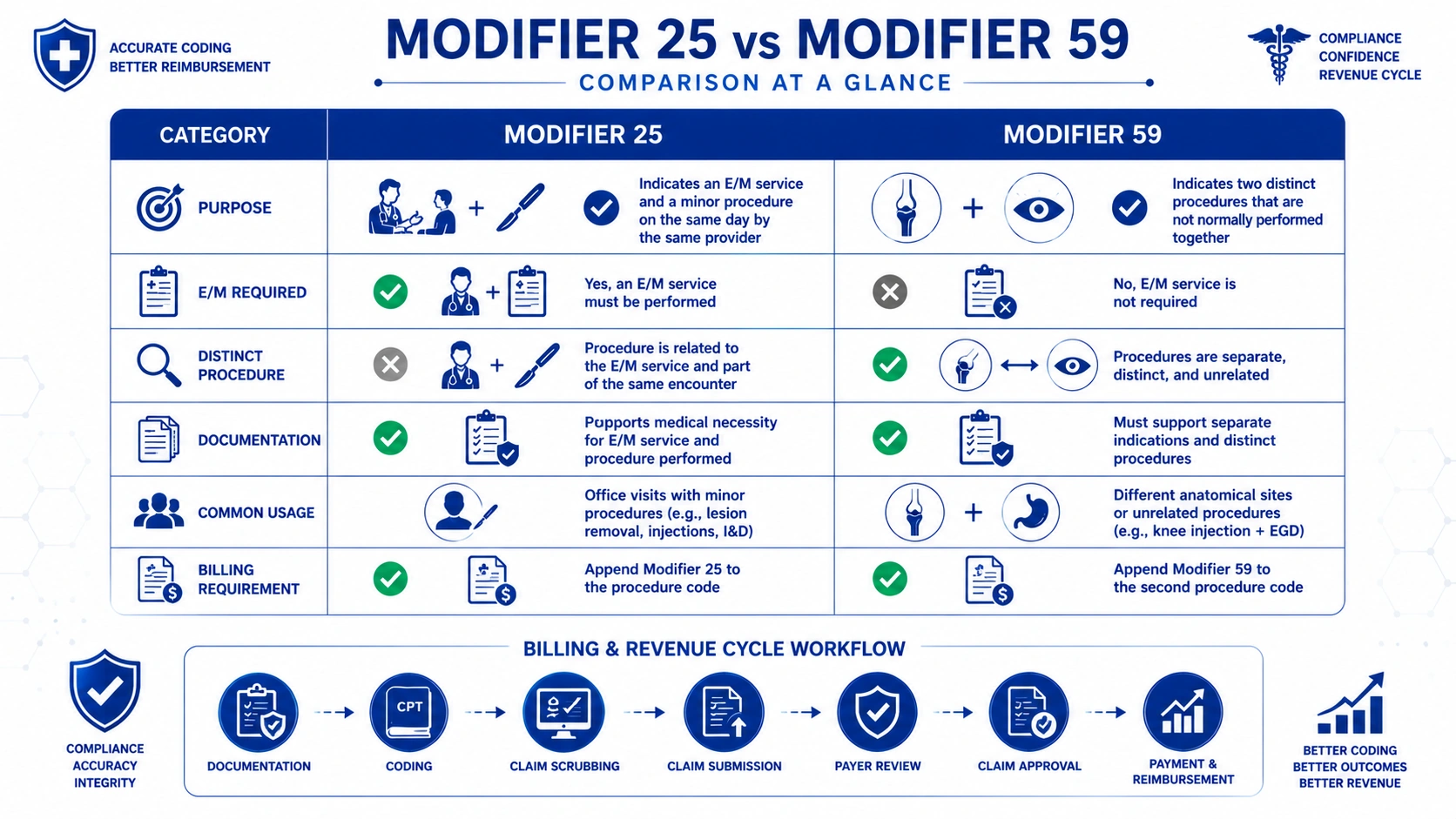
In the modifier 25 vs modifier 59 comparison, modifier 25 is appended to an E/M code to show a significant, separately identifiable evaluation service performed the same day as a procedure. Modifier 59 is appended to a non-E/M procedure code to show it is distinct or independent from another procedure billed the same day.
What Is Modifier 25?
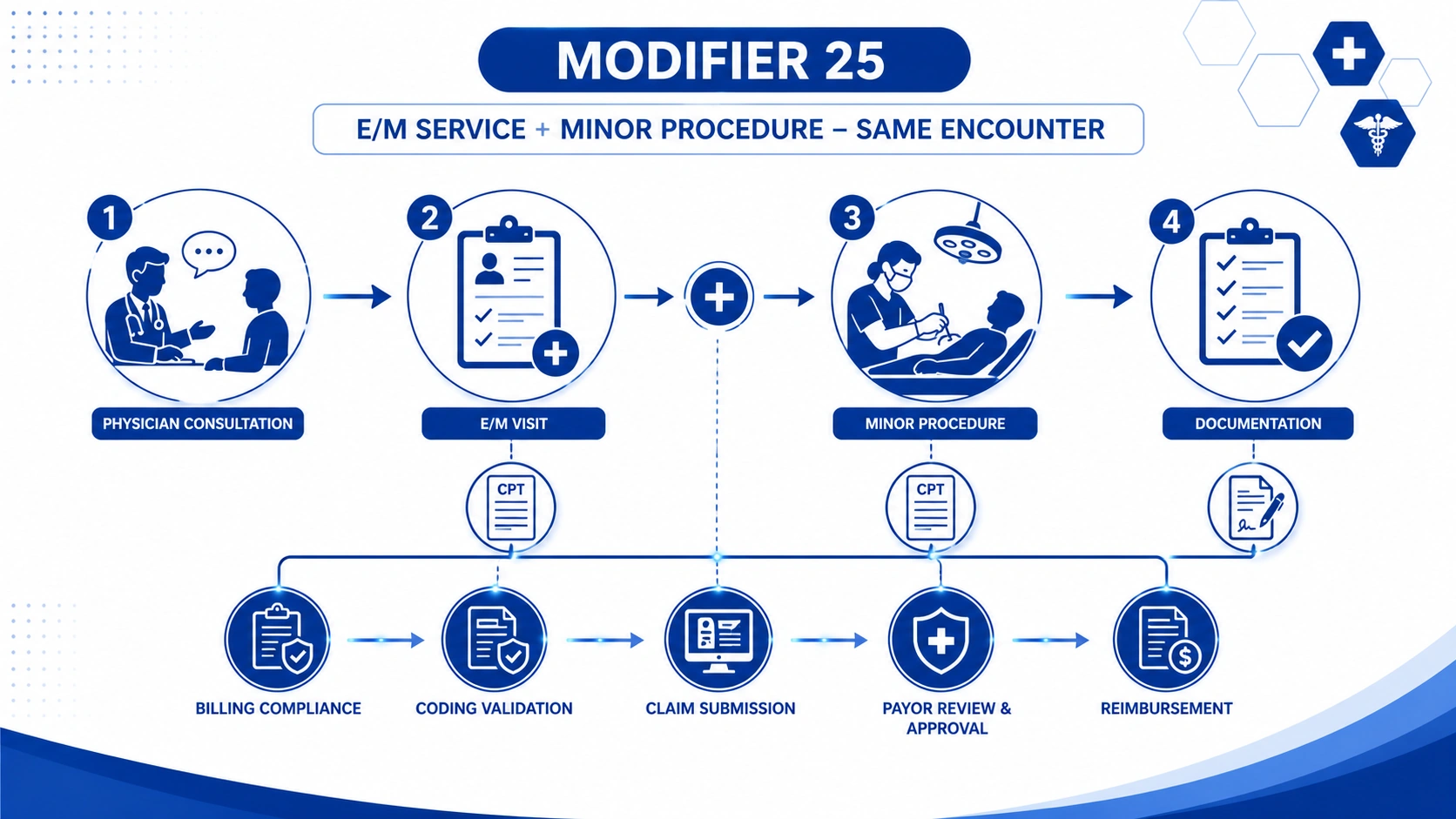
Modifier 25 belongs exclusively to Evaluation and Management (E/M) codes. It tells the payer that on the same day as a procedure or another service, the provider also performed a significant, separately identifiable E/M service — one that goes beyond the routine pre-procedure and post-procedure work already bundled into the procedure’s payment.
Think of a dermatology patient who comes in for a scheduled mole removal but also mentions a new, unrelated rash. If the physician evaluates and manages the rash as a distinct clinical problem, with its own history, exam, and medical decision-making, modifier 25 lets the practice bill for both the E/M visit and the procedure. Without it, the E/M gets bundled into the procedure and the visit goes unpaid.
Before/after example: A patient presents for a scheduled joint injection. The physician also evaluates new knee swelling unrelated to the injection site, documents a focused history and exam, and orders imaging. Billed correctly, this claim includes the injection code plus an E/M code with modifier 25, supported by a clearly separate note. Billed incorrectly — no modifier, or modifier 25 attached to a visit note that only restates the procedure indication — the E/M line denies as bundled.
What Is Modifier 59?
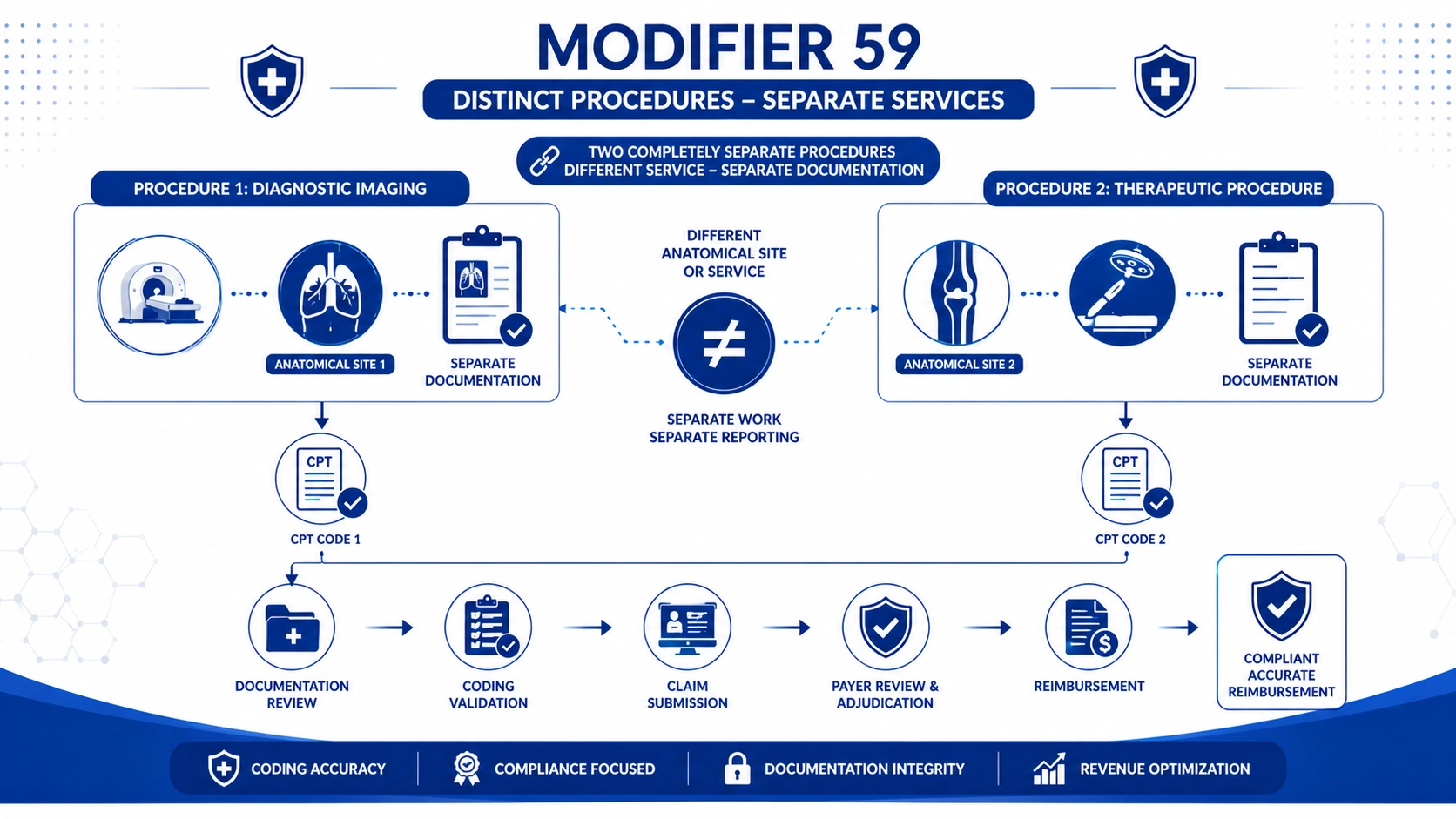
Modifier 59 is a distinct procedural service modifier, and it never touches an E/M code. It applies to non-E/M procedure codes to indicate that two procedures billed on the same date were performed at separate sites, separate sessions, or represent otherwise independent services that would normally be bundled under NCCI edits (National Correct Coding Initiative).
Before/after example: An orthopedic surgeon performs arthroscopic debridement on the knee and, later in the same session, treats a separate lesion on the same joint through a distinct incision. Billed correctly, the second procedure carries modifier 59 with operative notes clearly documenting separate anatomic sites. Billed incorrectly — modifier 59 applied by default to clear a bundling edit without documentation of a genuinely separate service — the claim is a compliance risk even if it initially pays.
Modifier 59 vs the X{EPSU} Modifiers
CMS introduced four more specific alternatives to modifier 59: XE (separate encounter), XS (separate structure), XP (separate practitioner), and XU (unusual non-overlapping service). These are collectively known as the modifier 59 subset codes, and CMS has stated a preference for their use whenever the more specific circumstance applies. Comparing modifier 59 vs XE XP XS XU, the difference is precision: modifier 59 is a general-purpose distinct procedural service modifier, while the X{EPSU} set tells the payer exactly why the services are separate. Many payers still accept modifier 59, but using the specific X modifier when it fits reduces the odds of a manual review and supports medical billing accuracy.
Modifier 25 vs Modifier 59 — Key Differences
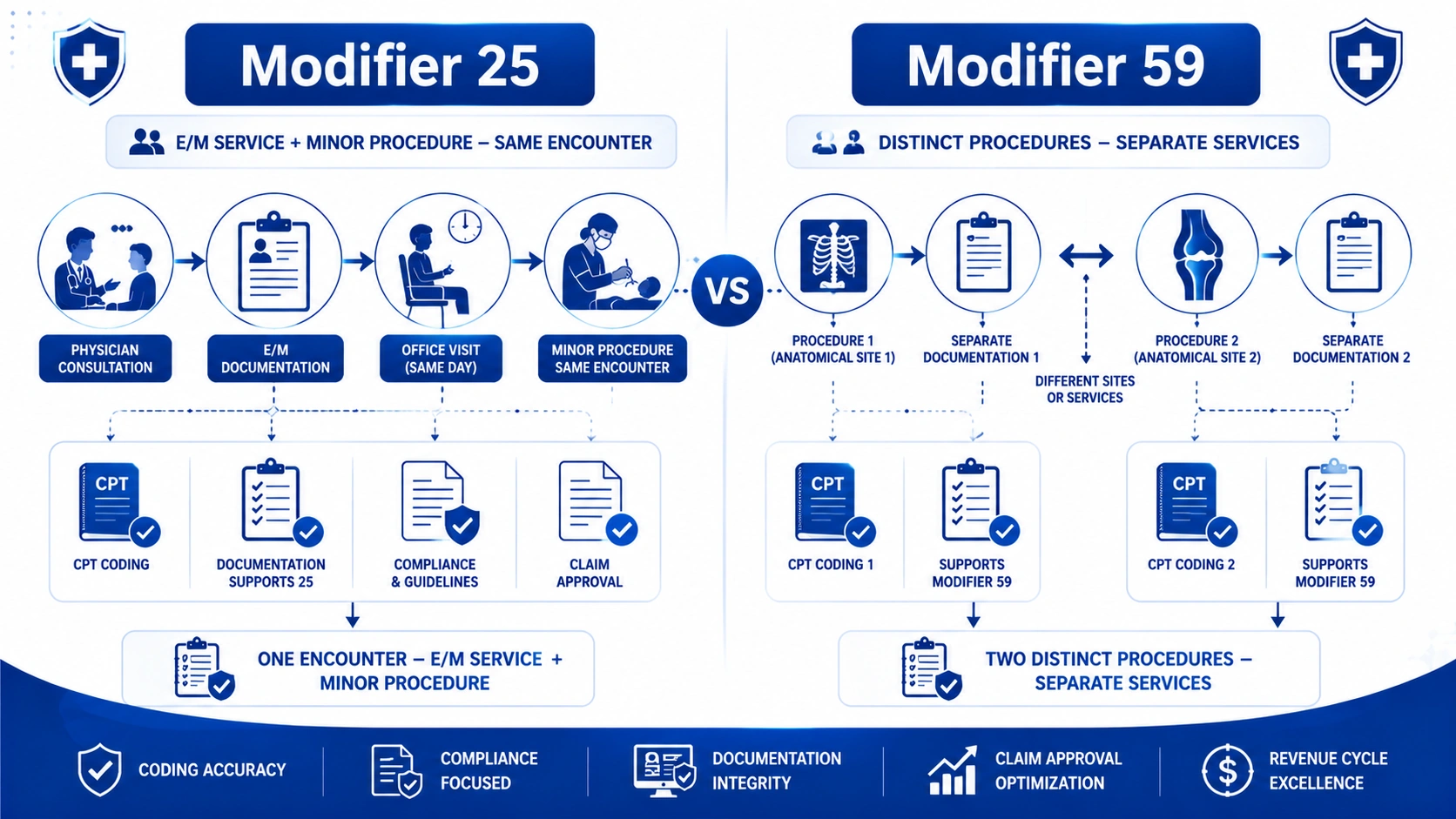
The core of the modifier 25 vs modifier 59 question comes down to code type. If you remember nothing else, remember this: modifier 25 rides on an E/M code, and modifier 59 rides on a procedure code. They solve different bundling problems and are never interchangeable.
E/M Codes vs Procedure Codes
Modifier 25 only ever attaches to an Evaluation and Management code — office visits, consults, and similar cognitive services. Modifier 59 only ever attaches to a procedural or diagnostic code that isn’t an E/M service. If your coder is debating whether to put modifier 59 on an office visit code, that’s the signal something has gone wrong upstream in the coding workflow.
Documentation Requirements for Each
Modifier 25 requires a note that stands on its own: a distinct history, exam, and medical decision-making process that isn’t already accounted for in the procedure’s global payment. Vague statements like “reviewed indication for procedure” won’t survive an audit. Modifier 59 requires operative or procedural documentation identifying separate anatomic sites, separate sessions, or separate incisions — not just two CPT codes that happened to be billed together. These documentation requirements are the single biggest driver of denials and post-payment recoupments tied to both modifiers, and they matter for coding compliance regardless of specialty.
Can You Use Modifier 25 and Modifier 59 Together?
Yes — modifier 25 and modifier 59 together are appropriate on the same claim when the clinical facts support both. Because modifier 25 always applies to the E/M line and modifier 59 always applies to a procedure line, they aren’t competing for the same code; they’re solving two separate bundling problems on the same date of service.
A common scenario: a physician performs a separately identifiable E/M service (modifier 25 on the E/M code) and also performs two distinct, non-E/M procedures at separate anatomic sites during the same visit (modifier 59 on the second procedure code). Each modifier needs its own supporting documentation. Using modifier 25 and modifier 59 together without separately justifying each one is a fast path to a denied claim or a flagged audit pattern.
Common Denial Reasons for Modifier 25 and 59
Most modifier-related denials trace back to the same root causes: a missing modifier, a modifier applied without adequate documentation, or a modifier applied automatically to bypass an NCCI edit rather than to reflect what actually happened in the encounter.
Modifier 25 Denials
The leading modifier 25 denial reasons include: E/M documentation that fails to stand apart from the procedure note, using modifier 25 for a routine pre- or post-procedure evaluation that’s already bundled, mismatching modifier 25 with a claim that actually requires modifier 57 (decision for surgery), and billing patterns that trigger payer-side statistical review because modifier 25 is applied on nearly every same-day procedure visit.
Modifier 59 Denials
Modifier 59 denials typically stem from applying the modifier without operative documentation of a separate site or session, using modifier 59 where a more specific X{EPSU} modifier was available and expected, and repeat unbundling patterns that draw scrutiny under procedure-to-procedure edits. Payers and auditors treat a high modifier 59 override rate as a red flag for systemic coding compliance problems, not just isolated errors.
Modifier 25 vs Modifier 59 — Side-by-Side Comparison
| Factor | Modifier 25 | Modifier 59 |
|---|---|---|
| Applies to | E/M codes only | Non-E/M procedure codes only |
| Purpose | Significant, separately identifiable E/M service | Distinct procedural service, separate from another procedure |
| Typical trigger | Office visit + same-day procedure | Two procedures normally bundled under NCCI |
| Documentation needed | Standalone history, exam, MDM | Separate site, session, or incision noted in op note |
| Common replacement/related codes | Modifier 57 (decision for surgery) | XE, XP, XS, XU |
| Highest audit risk specialty pattern | Dermatology, ophthalmology, urgent care | Orthopedics, general surgery, ASC multi-procedure cases |
| Can be used with the other modifier? | Yes, on the E/M line | Yes, on the procedure line |
Modifier 25 and 59 Denial Trends in 2026
The numbers behind modifier 25 vs modifier 59 errors are significant enough that most practices can’t afford to treat them as a back-office detail.
- The average initial claim denial rate sits at 11.8%, with more than 41% of providers now operating above a 10% denial rate, according to Experian’s 2025 State of Claims report and Kodiak Solutions/HFMA data.
- Industry audit data cited by AAPC shows unbundling errors — the core issue modifier 59 is meant to resolve — appear in roughly 15% of audited charts.
- A 2025 OIG audit of E/M services billed on the same day as eye injections found that 42% of those encounters used modifier 25, and documentation for the large majority of sampled claims did not support its use, putting $124 million in Medicare payments at risk of recoupment.
- A related OIG review found dermatology carried the highest modifier 25 usage rate of any specialty, alongside an estimated $62.9 million in overpayments tied to documentation, leveling, and modifier misuse.
- CMS continues to expand adoption of the X{EPSU} modifiers as the preferred, more specific alternative to modifier 59, with the 2026 NCCI Policy Manual reaffirming that payers should favor the specific X modifier whenever the circumstance fits.
These figures make the case plainly: modifier errors are not a minor coding footnote. They’re a measurable driver of claim denial rate and audit exposure across specialties.
Best Practices to Avoid Modifier-Related Denials
A short, repeatable documentation checklist prevents most modifier 25 and modifier 59 denials before they happen:
- Confirm the E/M note stands alone, with its own history, exam, and medical decision-making, before appending modifier 25.
- Never default to modifier 25 or modifier 59 just to clear a system edit — confirm the clinical documentation supports it first.
- Check whether a more specific X{EPSU} modifier applies before defaulting to modifier 59.
- Run every multi-procedure claim through an updated NCCI edit check prior to submission; CMS refreshes procedure-to-procedure edits quarterly.
- Audit high-frequency modifier 25 and modifier 59 users on a routine schedule, not just after a payer flags a pattern.
- Train providers directly — documentation gaps, not billing intent, cause most denials and recoupments tied to these modifiers.
Addressing clinical documentation errors at the source does more for your denial rate than any amount of after-the-fact appeal work; see our guide on clinical documentation errors for a deeper walkthrough.
How TMS Billings Helps Practices Get Modifier Coding Right
At TMS Billings, our coding and compliance team builds modifier accuracy directly into the claims workflow, not as an afterthought. We run pre-submission NCCI edit checks, verify that E/M documentation genuinely supports modifier 25 before a claim goes out, and confirm that modifier 59 or the appropriate X{EPSU} modifier is backed by clear operative documentation.
That level of review is part of how our Revenue Cycle Management Services keep denial rates down for multi-specialty practices with high same-day E/M and procedure volume — dermatology, orthopedics, cardiology, and urgent care among them. If you’re evaluating how modifier accuracy fits into your budget, our breakdown of medical billing pricing models explains how coding review is typically structured into a billing partnership.

Key Takeaways
- Modifier 25 attaches only to E/M codes; modifier 59 attaches only to non-E/M procedure codes.
- Modifier 25 requires a standalone, significant separately identifiable E/M service note.
- Modifier 59 requires documentation of a genuinely distinct procedure — separate site, session, or incision.
- Modifier 25 and modifier 59 together are appropriate when each modifier is independently supported by documentation.
- CMS favors the X{EPSU} modifiers over modifier 59 whenever the more specific circumstance applies.
- Both modifiers carry real audit risk — OIG data ties hundreds of millions of dollars in Medicare payments to documentation gaps tied to modifier 25 alone.
Final Thoughts
The modifier 25 vs modifier 59 decision isn’t complicated once you separate the two questions it actually answers: is this a separately identifiable E/M service, or is this a distinct procedure? Get that distinction right, document it consistently, and your coders will spend less time reworking denials and more time keeping claims clean the first time. If your practice is seeing a rising claim denial rate tied to modifier use, TMS Billings’ coding and compliance team can run a modifier-focused audit of your recent claims and show you exactly where the documentation gaps are — reach out to get started.


