Switching Medical Billing Providers Without Losing Claims: The 2026 Transition Checklist
Switching medical billing providers is one of the most consequential decisions your behavioral health practice will make. Get it right, and you unlock better collections, cleaner claims, and less administrative burden. Get it wrong, and your revenue cycle can spiral into denial chaos, aged AR, and cash flow disruption.
If your practice is ready to switch billing providers in 2026, you need more than a termination letter and a new contract. You need a structured transition plan that protects every claim, every dollar, and every patient encounter from the moment you notify your current vendor to the day your new partner achieves full operational velocity.
At TMS Billings, we’ve guided dozens of mental health practices through successful billing vendor transitions. This checklist reflects everything we’ve learned — the pitfalls, the non-negotiables, and the proven phases that separate a seamless handoff from a revenue disaster.
What Does It Mean to Switch Billing Providers?
Switching billing providers means transferring your medical billing operations from one revenue cycle management company to another. This transition involves moving patient data, claims history, accounts receivable, payer contracts, and fee schedules while ensuring continuous claim submission and payment collection without revenue interruption.
Why Practices Switch Billing Providers in 2026
Three converging forces are driving more practices than ever to switch billing providers this year.
First, the CMS Prior Authorization API rule went live in January 2026. Billers without API integration are still faxing prior authorizations that should now be electronic — adding six to nine days of unnecessary AR aging per authorized claim. If your current vendor hasn’t upgraded, they’re costing you time and money on every prior-authorized service.
Second, AI-driven payer denials have climbed roughly 23 percent year over year. Human-only denial teams simply cannot keep pace with the volume and complexity of modern payer behavior. Practices are watching their denial rates creep up two points per quarter while their biller insists “nothing has changed”. According to recent AMA physician survey data , administrative burden from billing vendor transitions is now a top-three concern for independent practices.
Third, OBBBA Medicaid reform rewrote eligibility verification rules in 19 states. Many legacy billers have not retrained their teams on new pre-claim workflows, leaving practices exposed to avoidable denials.
For behavioral health practices — where session-based billing, strict documentation requirements, and varying payer policies create unique challenges — these forces are particularly acute. The question isn’t whether to evaluate your billing partnership. The question is whether you can afford to wait.
The Hidden Costs of a Poorly Managed Billing Transition
How Much Revenue Do Practices Lose During a Billing Handoff?
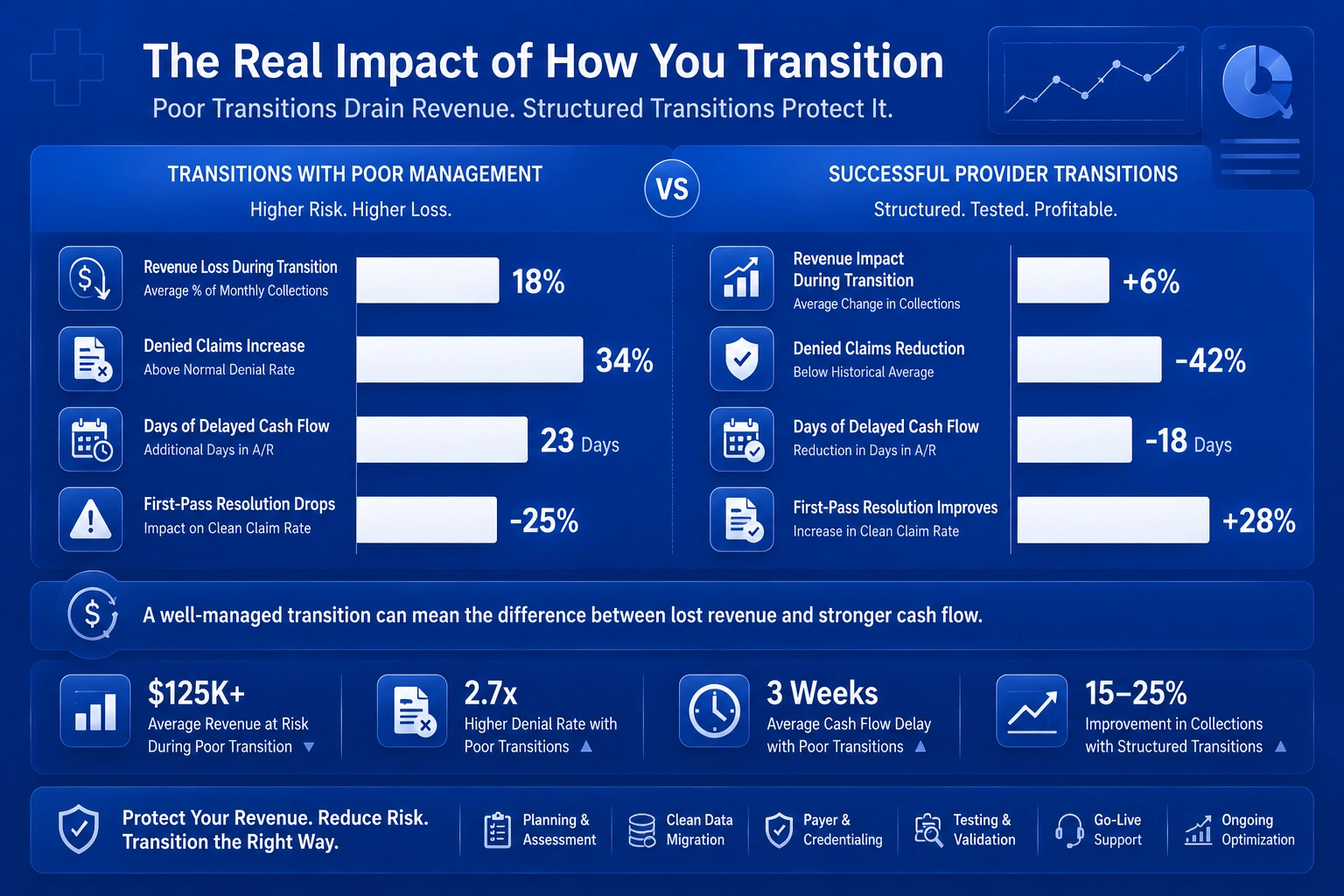
Most practices that switch medical billing companies lose 6 to 14 percent of revenue during the transition. This loss doesn’t happen because the new biller is worse. It happens because the handoff was structured wrong from day one.
For a behavioral health practice billing $3 million annually, a 10% revenue loss during transition represents **$300,000** in at-risk collections. That’s not a rounding error. That’s the difference between a profitable year and a stressful one.
The Domino Effect of Transition-Related Claim Denials
When you switch billing providers, your clean claim submission rates during transition often drop dramatically. Industry benchmarks from MGMA show first-pass claim acceptance sits at 95% or higher for high-performing practices. During a poorly managed transition, that rate can fall to 85% or below.
Each denied claim costs $25 to $118 in staff time to rework. And here’s the kicker: 65% of denied claims are never reworked at all. They become permanent revenue loss.
Why Data Gaps Are the #1 Cause of Transition Revenue Loss
The most common failure point in any billing vendor change is incomplete or corrupted data transfer. When patient demographics, insurance information, claims history, or AR aging reports don’t migrate cleanly, your new biller starts with a fractured view of your revenue cycle. Claims get submitted with errors. Payments get misapplied. Follow-up on aged AR falls through the cracks.
This is why a billing vendor change checklist must prioritize data integrity above all else.
The 6-Phase Medical Billing Provider Transition Checklist
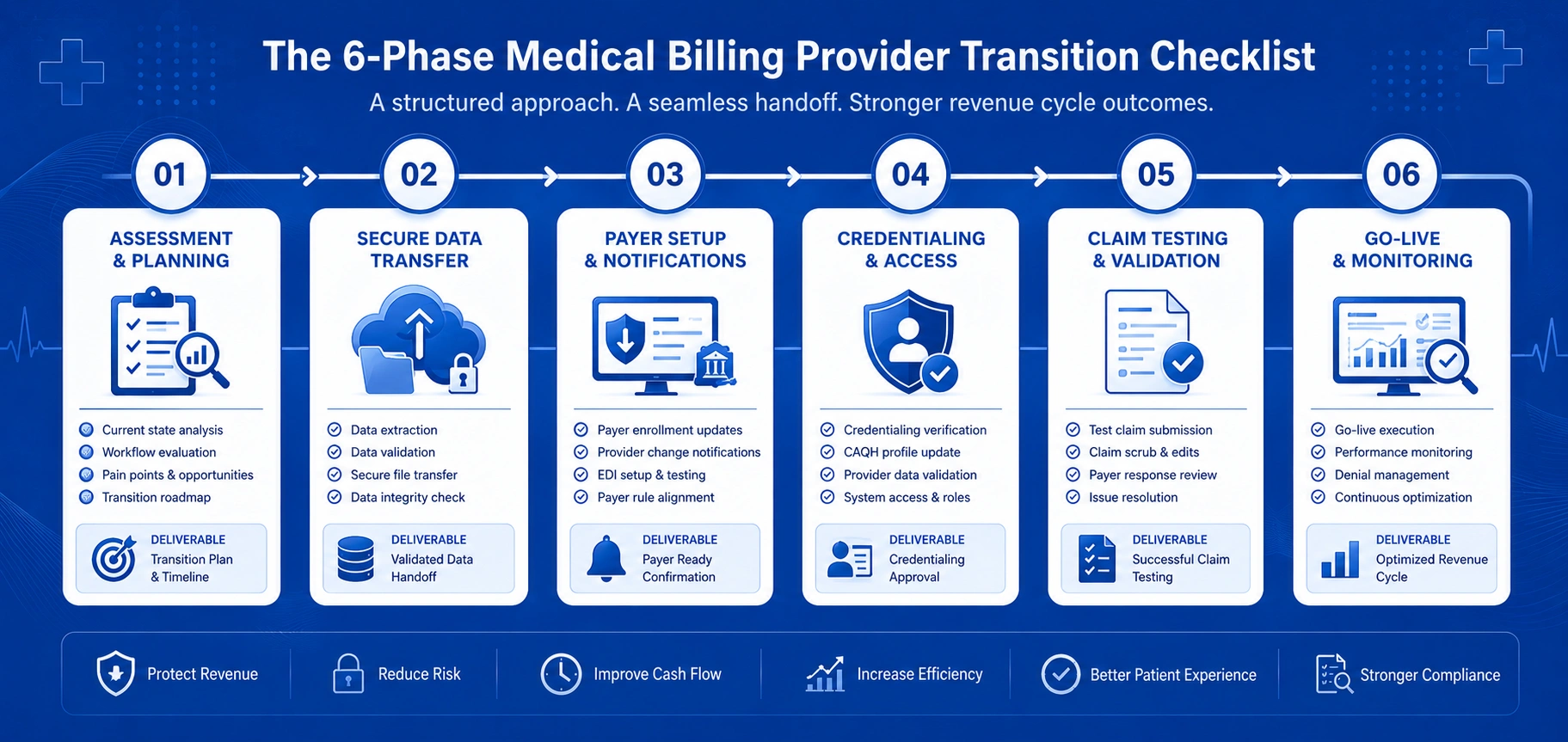
Phase 1: Pre-Transition Planning (60–90 Days Before Go-Live)
Your revenue cycle transition plan starts months before you submit your first claim through the new vendor. Begin by:
Auditing your current billing performance. Run your net collection rate, days in AR, denial rate, and first-pass resolution rate for the last 90 days. These numbers establish your baseline and help you measure the new vendor’s impact.
Reviewing your current contract. Understand termination notice periods, data export obligations, and any exit fees.
Identifying your transition team. Designate a practice lead who will coordinate between your current vendor, new vendor, and internal staff.
Setting clear success metrics. Define what “successful transition” looks like in measurable terms — e.g., first-pass rate above 92% within 30 days, AR over 90 days below 20%.
Phase 2: Data Audit and AR Inventory
Before you initiate the accounts receivable transfer medical billing process, you need a complete picture of what you’re moving.
Request from your current vendor:
Complete claims history for the last 12–24 months
AR aging reports by payer and by provider
Patient demographics with current insurance verification
Payer contracts and fee schedules
Authorizations for active treatment plans
This is also the time to identify any old AR recovery services opportunities — claims that were never paid and need aggressive follow-up before or after the transition.
Phase 3: Payer Notification and Revalidation
This is where many transitions fall apart. Payer enrollment revalidation when switching billers is not optional — it’s mandatory.
You must notify every commercial payer and Medicare of the billing provider change. This involves:
CMS billing provider change notification — submitting the appropriate CMS-855 forms and updating your Medicare enrollment records. Full guidelines are available directly from CMS.gov for Medicare billing provider change notification rules and reassignment of benefits requirements.
Medicare reassignment of benefits — ensuring all practitioners formally reassign their billing rights to the new billing entity’s Tax ID
Commercial payer credentialing timeline — initiating revalidation with each commercial payer, which can take 30 to 90 days depending on the payer
Start these notifications at least 60 days before go-live. Payers move slowly, and you cannot afford to have claims rejected because your enrollment isn’t active.
Phase 4: Technical Setup and Data Migration
Your new vendor needs to configure their system to match your practice’s workflows. This includes:
System-agnostic billing vendor transition — ensuring data moves cleanly regardless of whether your current and new vendors use different platforms
Mapping CPT codes, modifiers, and diagnosis codes to the new system
Setting up clearinghouse connections and payer IDs
Testing claim submission with sample files before going live
Phase 5: Parallel Billing and Claims Handoff
The claims handoff process is the most delicate phase of any medical billing provider transition.
Rather than flipping a switch and hoping for the best, run parallel billing for 30–60 days. Your current vendor continues submitting claims while your new vendor begins submitting a subset. This allows you to:
Compare clean claim submission rates during transition between both vendors
Identify and fix data mapping errors before they affect all claims
Build confidence in the new vendor’s processes
During this phase, denial management during billing handoff becomes critical. Both vendors should track denials separately so you can identify which denials are transition-related versus systemic.
Phase 6: Post-Transition Monitoring and Optimization
Once the new vendor is fully live, monitor performance closely for 60–90 days. Track:
First-pass claim acceptance rate benchmark — is it returning to 95%+?
Denial rates — are they trending up or down?
Days in AR — is the new vendor resolving claims faster?
Net collection rate — is revenue stabilizing or improving?
How to Protect Your Claims During the Handoff Process
Clean Claim Submission: What Changes During Transition?
When you switch billing providers, your claim submission process changes in several ways:
New clearinghouse — different editing rules, different rejection flags
New system workflows — different data entry points, different validation logic
New biller team — different familiarity with your specific payers and their quirks
These changes increase the risk of submission errors. The solution is rigorous testing — submitting sample claims, reviewing clearinghouse edits, and correcting issues before submitting live claims.
Denial Management During the Billing Handoff
Denial management during billing handoff requires proactive monitoring, not reactive firefighting. Your transition plan should include:
Daily denial reporting from both vendors during the parallel period
Root cause analysis for every transition-related denial — was it data, mapping, timing, or payer enrollment?
Escalation protocols for denials that threaten cash flow
Tracking Pending Claims Across Both Vendors
One of the biggest risks during a billing vendor transition is claims falling through the cracks. Create a master tracking log that includes:
Every claim submitted by your old vendor that is still pending payment
Every claim submitted by your new vendor
Every denial and appeal status
This log becomes your single source of truth during the handoff.
What Data Must Be Transferred When Switching Billing Vendors?
Patient Demographics and Insurance Information
Complete and accurate patient data is the foundation of clean claims. Ensure your new vendor receives:
Full patient names, DOBs, and contact information
Current insurance policy numbers and group IDs
Primary and secondary coverage details
Any coverage changes or updates from the last 12 months
Complete Claims History and AR Aging Reports
Your new biller cannot effectively manage your AR without knowing what’s already been billed, paid, denied, or appealed. Transfer:
All claims submitted in the last 24 months
Payment and adjustment history for each claim
AR aging by 30, 60, 90, and 120+ days
Denial reason codes and appeal status
Payer Contracts, Fee Schedules, and Authorizations
Your new vendor needs to bill at the correct contracted rates. Transfer:
All signed payer contracts
Current fee schedules for every payer and every service
Active authorizations for ongoing treatment plans
Any special payment arrangements or carve-outs
Payer Notifications and Credentialing Timeline
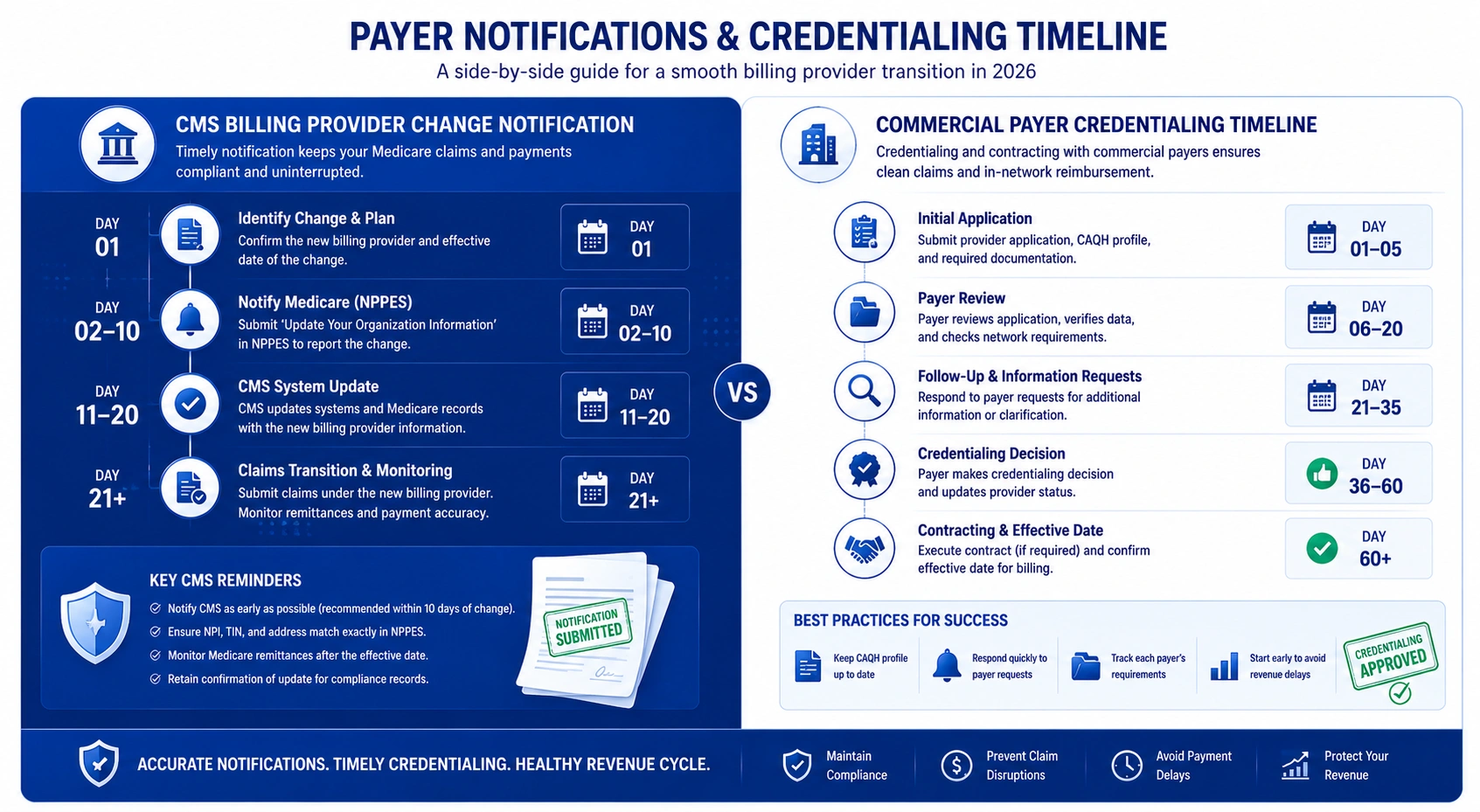
CMS Billing Provider Change Notification Requirements
The Centers for Medicare & Medicaid Services requires formal notification when you change billing arrangements. This typically involves:
Submitting CMS-855 enrollment forms for each billing provider
Updating your Medicare enrollment via PECOS (Provider Enrollment, Chain, and Ownership System)
Ensuring all practitioners who reassign benefits have current Medicare reassignment of benefits on file
Failure to complete these steps means Medicare will deny or return claims as unprocessable. For the most current forms and instructions, refer directly to CMS.gov .
Commercial Payer Credentialing and Revalidation Timelines
Commercial payers each have their own credentialing timeline for payer enrollment revalidation when switching billers:
| Payer Type | Typical Timeline | Key Action |
|---|---|---|
| Medicare | 30–60 days | CMS-855 + PECOS update |
| Major commercial (BCBS, United, Cigna, Aetna) | 30–90 days | Revalidation application |
| Medicaid (state-specific) | 45–90 days | State enrollment update |
| Regional payers | 30–60 days | Contract re-attestation |
Start every payer notification at least 60 days before go-live. Do not assume your new vendor can “figure it out” after the transition begins.
Medicare Reassignment of Benefits: What You Need to Know
Medicare reassignment of benefits is the formal process by which practitioners authorize their billing entity to receive Medicare payments on their behalf. When you switch billing providers, every practitioner who treats Medicare patients must reassign their benefits to the new billing entity’s Tax ID.
This is not optional. Beginning in 2026, Medicare will deny claims if reassignment is not properly recorded in PECOS. The reassignment application must be submitted for each physician or practitioner. Detailed rules are published on CMS.gov .
How Much Revenue Is Your Practice Losing to Transition Errors?
Example 1 — Lost Claims Due to Incomplete Data Transfer
A 5-provider behavioral health group decided to switch billing providers without conducting a full data audit. Patient insurance information for 200 active patients was incomplete in the transfer. The new vendor submitted 400 claims in the first month — and 35% were denied for eligibility or subscriber ID errors.
Each denied claim cost $47** to rework on average. The practice spent **$6,580 in staff time just to correct claims that should have been clean. Worse, 65% of those denials were never reworked, becoming $12,000+ in permanent revenue loss.
Example 2 — AR Write-Offs from Missed Follow-Up During Handoff
A psychiatry practice with $800,000 in outstanding AR initiated a medical billing provider transition without a clear plan for old AR recovery services. During the 45-day handoff, neither vendor took ownership of follow-up on 120-day+ claims.
Result: $47,000 in AR aged past timely filing limits and was written off as unrecoverable. That revenue was gone — not because payers denied it, but because no one followed up.
Example 3 — Denial Spike from Incorrect Payer Enrollment
A multi-provider LCSW practice switched medical billing companies but delayed payer enrollment revalidation when switching billers for three commercial payers. Claims submitted in the first 30 days were rejected as “provider not enrolled.”
The practice lost $28,000 in claims that had to be resubmitted after enrollment was complete — delaying payment by 60+ days and creating a cash flow crunch that strained operations.
How to Choose the Right New Billing Partner
Not every billing company is equipped to handle a system-agnostic billing vendor transition or manage the complexities of behavioral health revenue cycle. Before you sign, evaluate potential partners on:
Specialty expertise — Do they understand session-based billing, CPT codes for psychotherapy and psychiatric evaluation, and the specific documentation requirements of mental health claims?
Transition methodology — Do they have a documented billing vendor change checklist and transition team?
Technology stack — Can they integrate with your EHR? Do they offer API-based prior authorization?
Performance guarantees — Will they commit to specific first-pass claim acceptance rate benchmark targets?
References — Talk to other behavioral health practices that have made the switch.
Documentation Requirements for a Smooth Transition
What Your Current Vendor Must Provide Before Termination
Before you terminate your current vendor, demand:
Complete claims data export in a usable format
AR aging reports with full detail by payer and patient
Copies of all payer contracts and fee schedules
Denial logs with reason codes for the last 12 months
Clearinghouse credentials and connection details
What Your New Vendor Needs to Start Billing Immediately
Your new vendor cannot begin billing without:
Complete patient demographic and insurance data
Payer enrollment confirmation for Medicare and all commercial payers
Fee schedules loaded and verified
Clearinghouse connection established and tested
Sample claims submitted and accepted
Contracts and Service-Level Agreements: What to Look For
Your contract with the new vendor should specify:
Net collection rate target (aim for 95%+ for behavioral health)
Days in AR target (35 days or fewer)
Denial rate cap (5% or less)
First-pass resolution rate (92% or higher)
Reporting frequency and format
Transition support — dedicated project manager, training, and go-live support
Strategies Every Practice Should Implement Right Now
Audit Your Current Billing Performance Before You Switch
Run these five numbers from your last 90 days:
| Metric | Healthy | Switch Signal |
|---|---|---|
| Net Collection Rate | ≥ 96% | < 93% |
| Days in AR | ≤ 35 | > 45 |
| First-Pass Resolution Rate | ≥ 92% | < 85% |
| Denial Rate | ≤ 5% | > 8% |
| AR > 90 days | < 15% | > 25% |
If three or more land in the “Switch Signal” column, switching is the higher-yield path.
Establish a Dedicated Transition Team
Assign one internal lead to coordinate the transition. This person becomes the single point of contact for your current vendor, new vendor, and internal staff. Without a dedicated lead, communication breaks down and claims fall through the cracks.
Create a 60-Day Parallel Billing Buffer
Do not terminate your current vendor until your new vendor has demonstrated clean claim submission for at least 30 days. A 60-day parallel billing buffer gives you time to identify and fix issues without disrupting cash flow.
Train Staff on New Workflows and Systems
Your front desk, clinicians, and billing staff all need training on new processes. Schedule training sessions before go-live and provide reference materials for common tasks.
Outsource Your Transition to RCM Specialists
If your practice lacks the internal resources to manage a billing vendor transition, consider outsourcing the transition to RCM specialists. Firms like TMS Billings offer dedicated transition teams that handle data migration, payer notifications, parallel billing, and post-transition monitoring — so your practice can focus on patient care.
How Outsourced RCM Support Protects Your Revenue During Transition
Outsourcing your medical billing provider transition to an experienced RCM partner provides several advantages:
Dedicated transition project managers who have guided dozens of practices through vendor changes
Proven billing vendor change checklist methodologies that prevent common pitfalls
Data migration expertise — ensuring clean, complete data transfer
Payer notification coordination — managing CMS, Medicare, and commercial payer revalidation
Denial management during billing handoff — proactive monitoring and rapid resolution
Performance benchmarking — tracking first-pass claim acceptance rate and other KPIs throughout the transition
The cost of outsourcing is far less than the 6–14% revenue loss that plagues poorly managed transitions.
How TMS Billings Helps Practices Switch Billing Providers Seamlessly
At TMS Billings, we specialize in helping behavioral health practices switch billing providers without losing revenue. Our transition approach includes:
Comprehensive pre-transition audit — we analyze your current performance and identify the gaps your new vendor must address
End-to-end data migration — we ensure every patient record, claim, and AR dollar moves cleanly
Payer enrollment management — we handle CMS billing provider change notification, Medicare reassignment of benefits, and commercial payer revalidation
60-day parallel billing — we run alongside your current vendor to ensure continuity
Post-transition performance monitoring — we track clean claim submission rates during transition, denial rates, and AR resolution to ensure you’re on track
Our team understands the unique challenges of behavioral health billing — from psychotherapy and psychiatric evaluation codes to crisis billing and the specific documentation requirements of mental health claims.

Explore our Revenue Cycle Management Services to learn how we protect your revenue during and after a vendor transition. Our Medical Billing Services and Medical Coding Services are designed specifically for behavioral health practices that demand accuracy, transparency, and results.
The Financial Cost of a Poorly Executed Billing Transition
The data on billing vendor transitions is clear: poor execution is expensive. According to benchmarks from MGMA and the AMA , the financial impact is well-documented.
| Statistic | Data Point | Source |
|---|---|---|
| Practices that lose revenue during transition | Most practices that switch billing companies experience revenue loss | Industry benchmark data |
| Average revenue loss during a poorly managed handoff | 6–14% of revenue | Medical Billers and Coders |
| Cost to rework a denied claim | $25–$118 per claim | MGMA / HFMA |
| First-pass claim acceptance benchmark | 95%+ (drops during transition) | MGMA |
| Net collection rate gap | High-performing practices achieve 95–98% NCR; underperformers fall below 90% | Industry benchmarks |
When you consider that a 7 percentage-point NCR improvement — from 87% to 94% — equals **$700,000** in additional annual collections on a $10M billing volume, the financial case for a well-executed transition becomes undeniable.
Key Takeaways
Most practices lose 6–14% of revenue during a billing vendor transition — but this loss is preventable with proper planning.
Start your transition 60–90 days before go-live to allow time for data audit, payer notifications, and parallel billing.
Payer enrollment revalidation when switching billers is non-negotiable — start Medicare and commercial payer notifications early. Refer to CMS.gov for official Medicare rules.
Run parallel billing for 30–60 days to protect clean claim submission rates during transition.
Track first-pass claim acceptance rate and denial rates closely during and after the handoff.
Choose a new billing partner with behavioral health expertise, a documented transition methodology, and performance guarantees.
Outsource your transition to RCM specialists if your practice lacks internal transition resources.
Final Thoughts
Switching billing providers is not a decision to take lightly — but staying with an underperforming vendor is its own kind of risk. If your net collection rate has been below 93% for two consecutive quarters, your days in AR exceed 45, or your denial rate is above 8%, you’re not deciding whether to switch. You’re deciding how much longer you can afford to wait.
The 2026 billing landscape is more demanding than ever. AI-driven payer denials, new CMS prior authorization rules, and state-level Medicaid reforms are raising the bar for billing performance. Practices that switch billing providers with a structured transition plan will gain a competitive advantage. Those that don’t will continue to leak revenue.