Orthopedic Prior Authorization: Step-by-Step Process & Common Mistakes (2026)
If you run an orthopedic practice, you already know that getting paid isn’t just about delivering great care — it’s about navigating a maze of payer rules before the patient ever walks into the OR. Orthopedic prior authorization is one of the most time-consuming, documentation-heavy processes in all of healthcare billing, and the stakes keep getting higher every year. A single missed step can delay surgery by weeks, frustrate patients, and cost your practice thousands in lost or denied revenue.
Our team at TMS Billings works exclusively with orthopedic providers, and we’ve seen firsthand how orthopedic billing services built around a disciplined prior auth workflow can transform a practice’s financial health. For broader context on how payers are tightening prior authorization requirements industrywide, the American Medical Association’s prior authorization resources offer a sobering look at where things are headed. This guide walks you through every step of the process, every common mistake, and everything your team needs to do differently in 2026.
Why Orthopedic Prior Authorization Matters More Than Ever
The volume of procedures requiring prior authorization has grown significantly over the past several years, and orthopedic surgery is squarely in the crosshairs. Insurers now require pre-approval for a wide range of services — from total knee replacements and rotator cuff repairs to spinal fusions and arthroscopic procedures. According to the American Academy of Orthopaedic Surgeons, orthopedic procedures consistently rank among the most frequently denied and delayed due to prior authorization failures.
What does that mean for your practice? Delayed surgeries. Unhappy patients. Increased administrative burden. And, often, revenue that never makes it to your bank account.
Prior authorization requirements for orthopedic surgery aren’t going away — they’re getting stricter. Payers are demanding more detailed medical necessity documentation, tighter alignment between CPT codes on auth requests and actual claims, and faster turnaround on appeals when denials happen. If your front-end revenue cycle process isn’t keeping pace, denials will pile up.
Orthopedic revenue cycle management starts well before a claim is submitted. It starts the moment a patient is scheduled for a procedure. Getting prior auth right at that stage protects everything downstream.
The Complete Orthopedic Prior Authorization Process Step by Step
There’s no shortcut here. The prior auth process for orthopedic surgery has multiple distinct steps, and skipping or rushing any one of them is how denials happen. Here’s how the process should work from start to finish.
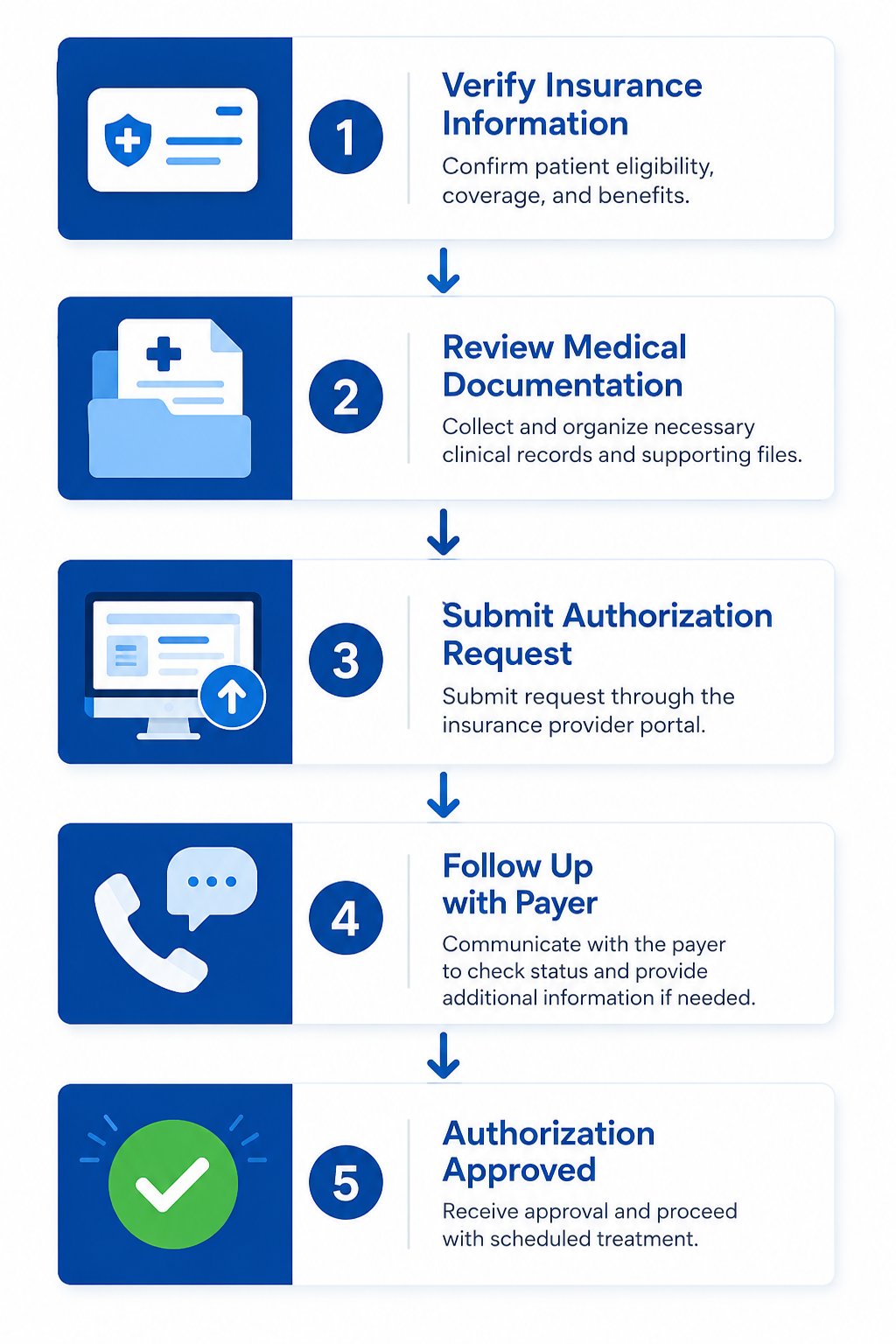
Step 1: Verify Patient Insurance & Benefits
Before anything else, your team needs to confirm the patient’s active coverage and understand exactly what their plan requires. Insurance eligibility verification for orthopedic patients isn’t just a checkbox — it’s the foundation of the entire authorization workflow.
Check the patient’s primary and secondary insurance. Confirm that the specific procedure is a covered benefit. Identify whether a referral is required before the authorization can even be submitted. Look at deductibles, out-of-pocket maximums, and any plan-specific payer authorization guidelines for orthopedic procedures. Some plans have very specific step therapy requirements — for example, requiring documented conservative treatment (physical therapy, injections) before approving a joint replacement.
If you skip this step or rush through it, you may spend hours preparing an authorization request for a plan that requires a referral first, or for a benefit that isn’t covered at all.
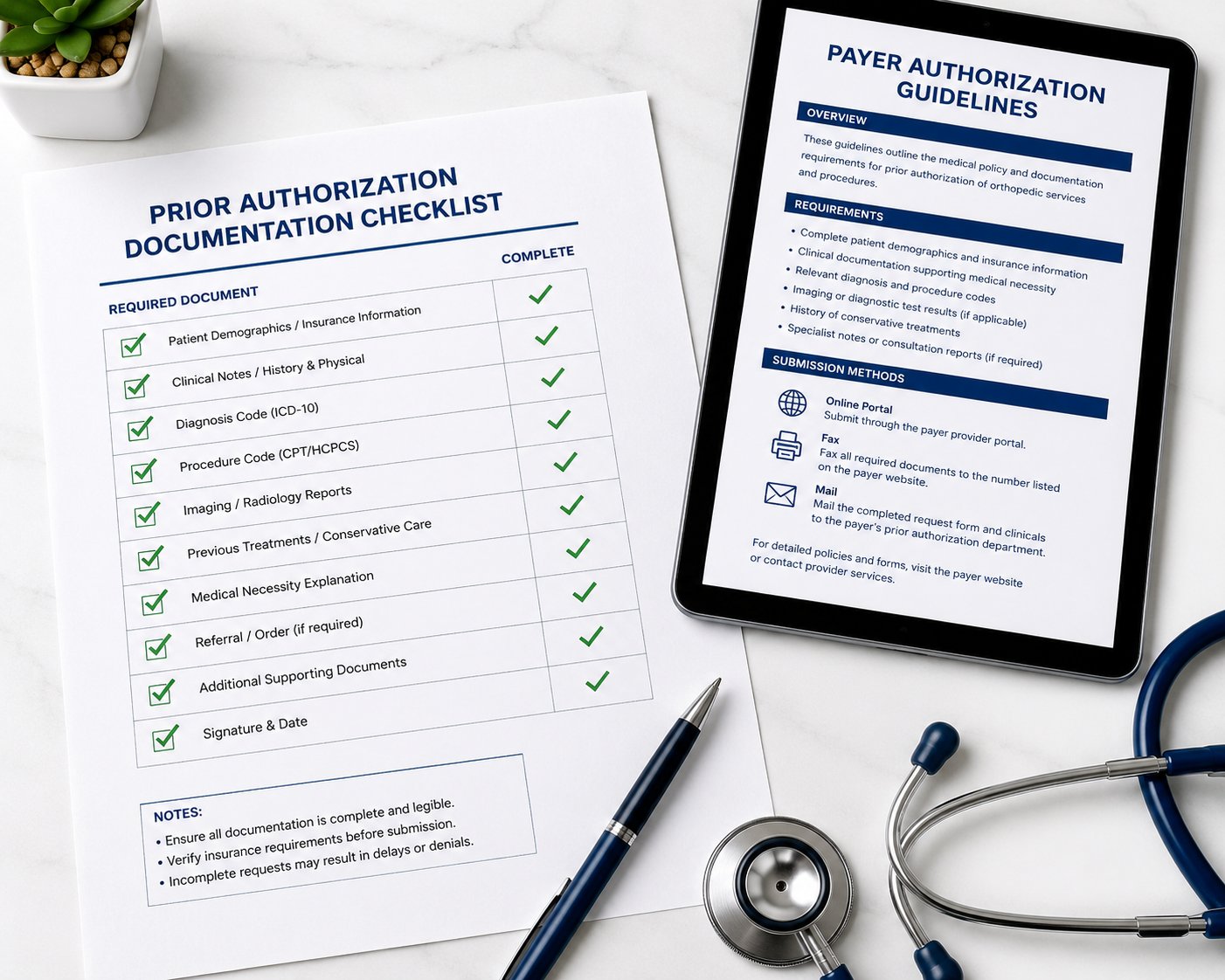
Step 2: Gather Medical Necessity Documentation for Orthopedic Cases
This is where most prior auth requests either succeed or fall apart. Payers don’t approve procedures — they approve documented medical necessity. Every piece of clinical evidence needs to be in order before the request goes out.
Medical necessity documentation for orthopedic procedures typically includes: office visit notes documenting the patient’s symptoms and functional limitations, imaging reports (X-rays, MRIs, CT scans), prior treatment history and its outcomes, referring physician notes if applicable, and the specific diagnosis codes and CPT coding for orthopedic procedures that will be performed.

Payers compare what you submit against their own clinical criteria. If the documentation doesn’t clearly show that the patient tried and failed conservative treatment, or that the procedure is medically necessary based on objective findings, the authorization will be denied. Be specific. Use language that mirrors payer clinical guidelines. Vague notes like “patient has knee pain” don’t cut it in 2026.
Step 3: Submit the Prior Authorization Request
Once documentation is complete, submit the authorization request through the payer’s preferred channel — online portal, fax, or phone, depending on the insurer. Include the correct CPT codes, the diagnosis codes, supporting clinical documentation, and the anticipated date of service.
One detail that causes endless problems: make sure the requesting provider information, facility information, and service codes on the authorization request exactly match what will appear on the eventual claim. Any mismatch — even a small one — creates a gap the payer can use to deny payment later.
Some payers have specific forms for orthopedic surgery prior authorization. Use them. Don’t improvise with a generic form when a plan-specific one exists.
Step 4: Follow Up With the Payer
Submitting the request is not the end of your responsibility — it’s the middle of it. Payers regularly lose faxes, have portal glitches, or let requests sit in a queue without action. Your team should follow up within 48–72 hours of submission to confirm the request was received and is being processed.
Tracking turnaround time matters. Urgent cases may qualify for expedited review, but you have to ask for it. Document every follow-up call — the date, the representative’s name, and what they told you. This documentation can be critical if you later need to appeal a denial or dispute a timely filing issue.
Step 5: Confirm Authorization Before Surgery
Once the authorization comes through, the work isn’t over. Confirm that the authorization number is valid, that it covers the specific procedure codes you plan to bill, and that it hasn’t already expired. Authorization approval for orthopedic surgery usually comes with an expiration date, and scheduling delays can push surgery past that window.
Also confirm that the authorization covers the correct facility. An auth granted at one surgical center doesn’t automatically transfer to another location. This is a detail that gets missed more often than you’d think.
Common Prior Authorization Mistakes That Delay or Deny Orthopedic Surgery
Knowing the steps isn’t enough if the execution is sloppy. These are the specific mistakes we see most often — and the ones that cost practices the most revenue.
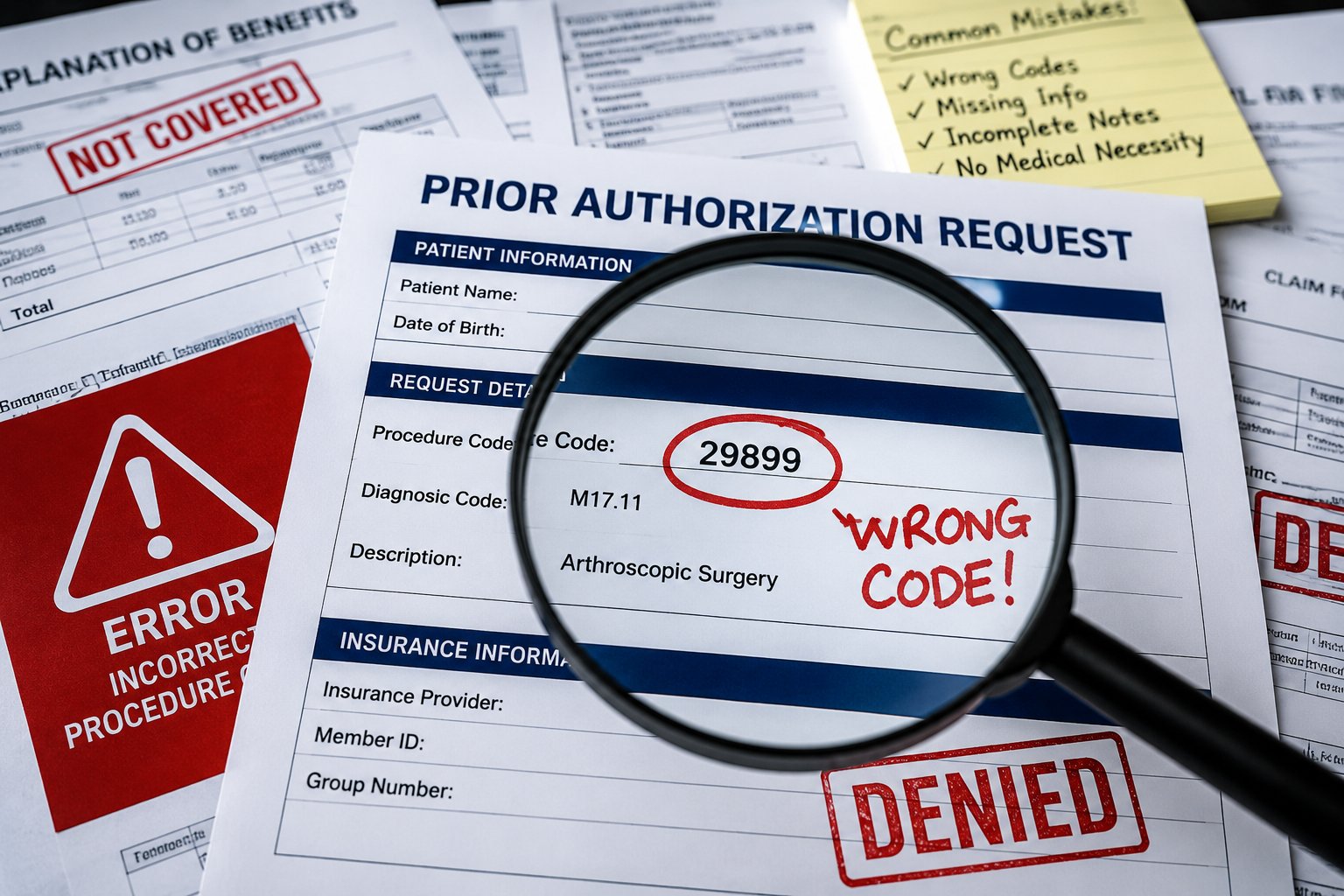
Wrong Procedure Code on Auth Request
CPT coding for orthopedic procedures can be complex. A surgeon may plan a primary knee replacement and submit the auth for that code, but intraoperatively decide to perform a revision or add a component. If the claim goes out with a different code than the authorization number covers, the payer has grounds to deny it.
Always align the authorized CPT codes with the expected surgical plan. If the plan changes before surgery, get the authorization updated before the date of service — not after.
Incomplete Medical Necessity Documentation for Orthopedic Cases
This is the single most common reason prior authorization is denied for orthopedic procedures. The clinical notes are vague. The imaging reports aren’t included. There’s no documentation of conservative treatment failure. The payer can’t establish medical necessity from what you sent, so they deny.
Checklists help. Before any authorization request goes out the door, have a standard documentation checklist specific to procedure type. Total joint replacements have different documentation requirements than arthroscopic procedures or spinal surgeries. Treat each one accordingly.
Missing Auth Before Scheduling
This happens in busy practices where clinical staff and scheduling staff aren’t fully aligned. A surgeon sees a patient, determines surgery is needed, and the patient gets scheduled before the auth process even begins. Then the auth takes longer than expected, or gets denied, and now you have a surgery date with no coverage and a frustrated patient.
Prior authorization requirements for orthopedic surgery must be initiated at the time of scheduling — not the day before. Build that workflow into your scheduling process so it’s impossible to book a surgery without triggering the auth request.
Not Updating Auth When Surgical Plan Changes
Patients’ conditions evolve. A planned arthroscopic procedure turns into an open repair. A unilateral case becomes bilateral. When the surgical plan changes after authorization has been obtained, the authorization must be updated to reflect the new scope of work.
Billing a service that doesn’t match the authorization is one of the clearest paths to an orthopedic claim denial. Payers audit for exactly this kind of discrepancy.
Why Is Prior Authorization Denied for Orthopedic Procedures?
Prior auth denial for orthopedic cases almost always traces back to a handful of root causes. Understanding them helps you prevent them.
Insufficient medical necessity is the most common reason. If the documentation doesn’t clearly establish that the patient meets the payer’s clinical criteria for the requested procedure, denial is automatic. The payer doesn’t have to prove the procedure is unnecessary — they just have to show you didn’t prove it is necessary.
Wrong or mismatched codes are the second major cause. The procedure code on the auth request doesn’t match the anticipated claim. The diagnosis code doesn’t align with the clinical documentation. Even minor discrepancies trigger denials.
Failure to follow plan-specific requirements is another. Some payers require second surgical opinions before approving joint replacement. Others require specific diagnostic criteria that must be explicitly referenced in your documentation. If you don’t know the payer’s specific requirements going in, you’re guessing — and guessing costs money.
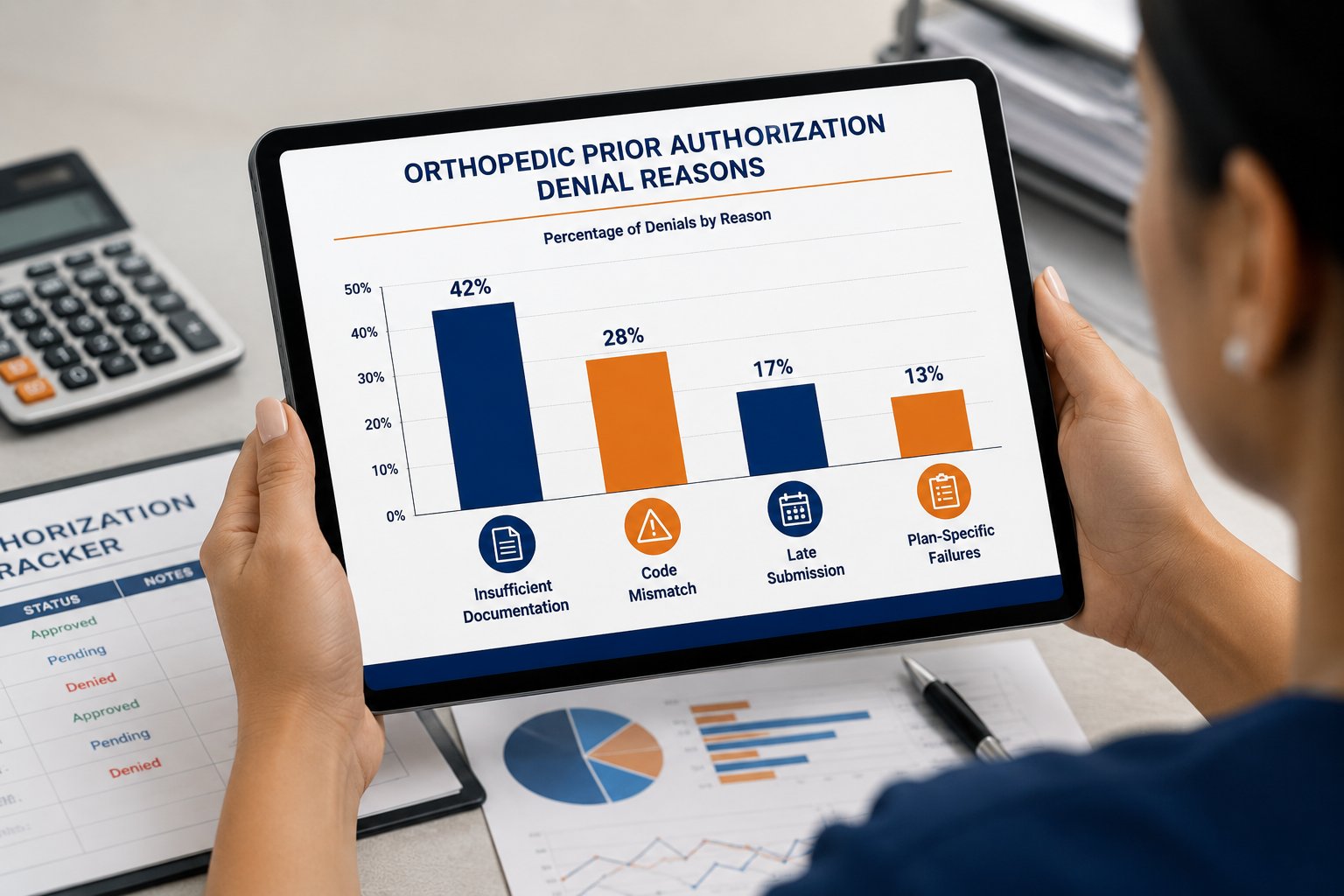
Finally, late submission is a growing problem. Many plans have windows within which prior authorization for elective orthopedic surgery must be submitted. Missing that window — even by a day — can mean starting the process over from scratch.
How to Appeal an Orthopedic Prior Authorization Denial
A denial isn’t the end — but how you handle it matters. Here’s how to appeal an orthopedic prior authorization denial effectively.
First, get the denial in writing and read it carefully. The denial letter tells you exactly why the payer said no. That’s your roadmap for the appeal. If the denial says insufficient medical necessity, your appeal needs to address that directly with additional clinical evidence. If it says the procedure isn’t covered, you may need to verify the patient’s specific plan benefits before proceeding.
Submit the appeal promptly. Most payers have strict deadlines — typically 30 to 60 days from the date of denial — and missing the appeal window forfeits your right to challenge the decision.
Include a physician attestation letter. When your surgeon writes directly to the medical director explaining the clinical rationale for the procedure, appeals have a meaningfully higher success rate than when documentation alone is submitted.
Reference the payer’s own clinical criteria in your appeal. Show that the patient’s case meets the criteria — point by point. Don’t make the reviewer work to find the connection. Lay it out clearly.
The Centers for Medicare & Medicaid Services outlines the formal appeal rights and timelines for Medicare patients — a useful reference for practices dealing with Medicare Advantage plan denials.
If the internal appeal fails, external review is often available. Patients have rights too, and sometimes engaging the patient in the appeal process — particularly through their state insurance commissioner — can accelerate resolution.
How TMS Billings Handles Prior Authorization for Orthopedic Practices
At TMS Billings, prior authorization isn’t a side task — it’s a core part of how we manage orthopedic revenue cycle management from end to end. Our team works exclusively with orthopedic providers, which means we know the payer-specific requirements, the documentation standards, and the CPT coding nuances that generalist billing companies miss.
When a patient is scheduled for surgery, our team initiates the insurance eligibility verification and authorization process immediately. We don’t wait. We use documented checklists for every procedure type, verify auth numbers before the date of service, and track every open authorization through to completion.
When denials happen — and in orthopedics, they do happen — we handle the appeal process with clinical input from your team and a clear, evidence-based submission strategy. We don’t let denials age. We work them fast.
If you’re losing revenue to prior auth denials, duplicate work, or authorization-to-claim mismatches, our orthopedic RCM solutions are built specifically to solve those problems.
Orthopedic Prior Authorization Best Practices for 2026
Payers are tightening their prior authorization requirements for orthopedic surgery heading into 2026, and practices that rely on informal or inconsistent processes will feel it in their denial rates. Here’s what orthopedic billing best practices look like right now.
Invest in payer-specific knowledge. Know which payers in your market require step therapy, which have specific forms, and which have the fastest turnaround times for urgent cases. That knowledge has real dollar value.
Standardize your documentation templates. Don’t let clinical staff submit whatever they happen to have on hand. Build templates for your most common procedures that prompt the documentation payers actually require — functional limitations, imaging findings, conservative treatment history.
Track your authorization data. Know your approval rate by payer, your average time-to-decision, and your appeal success rate. If a specific payer is denying 40% of your authorization requests, that’s a problem to solve — either through better documentation, direct payer outreach, or a peer-to-peer review strategy.
Train your front desk and scheduling staff on prior authorization requirements for orthopedic procedures. They’re the first line of the process. If they don’t understand why auth matters — or what triggers the need for one — errors will happen upstream of billing.
Build in a pre-surgery auth confirmation step. The day before every scheduled orthopedic surgery, someone on your team should verify the authorization is active, matches the planned procedure, and hasn’t expired.
Ready to Stop Losing Revenue to Prior Auth Denials?
Orthopedic prior authorization is one of the most document-intensive, time-sensitive administrative processes your practice manages — and it has a direct, measurable impact on your revenue. Every denial represents a procedure your surgeons performed that didn’t get paid, or a surgery that got delayed because the paperwork wasn’t in order.
The good news: with the right processes and the right team, prior auth doesn’t have to be a revenue leak. It can be a well-managed workflow that protects your practice and your patients.
Our team at TMS Billings has helped orthopedic practices across the country reduce denial rates, shorten authorization timelines, and build billing workflows that scale with their surgical volume. If prior authorization is creating bottlenecks or costing your practice money, we’d love to show you what a better process looks like.
Visit our orthopedic billing services page to learn more or schedule a consultation with our team. No pressure — just a straightforward conversation about where your revenue cycle stands and what it could look like.