
If your practice offers transcranial magnetic stimulation, you already know that getting paid for it is its own specialty. Denial rates are high, payer rules are inconsistent, and one miscoded session can unravel an entire 36-session treatment course. Understanding TMS CPT codes 2026 is not optional — it is the foundation of a financially healthy TMS program. This TMS billing guide 2026 was built specifically for psychiatrists, billing staff, and practice managers who need to stop leaving reimbursement on the table. Our Revenue Cycle Management Services team created this resource to walk you through every code, every rule, and every denial pattern you need to know right now.
What Are TMS CPT Codes in 2026?
What Are TMS CPT Codes?
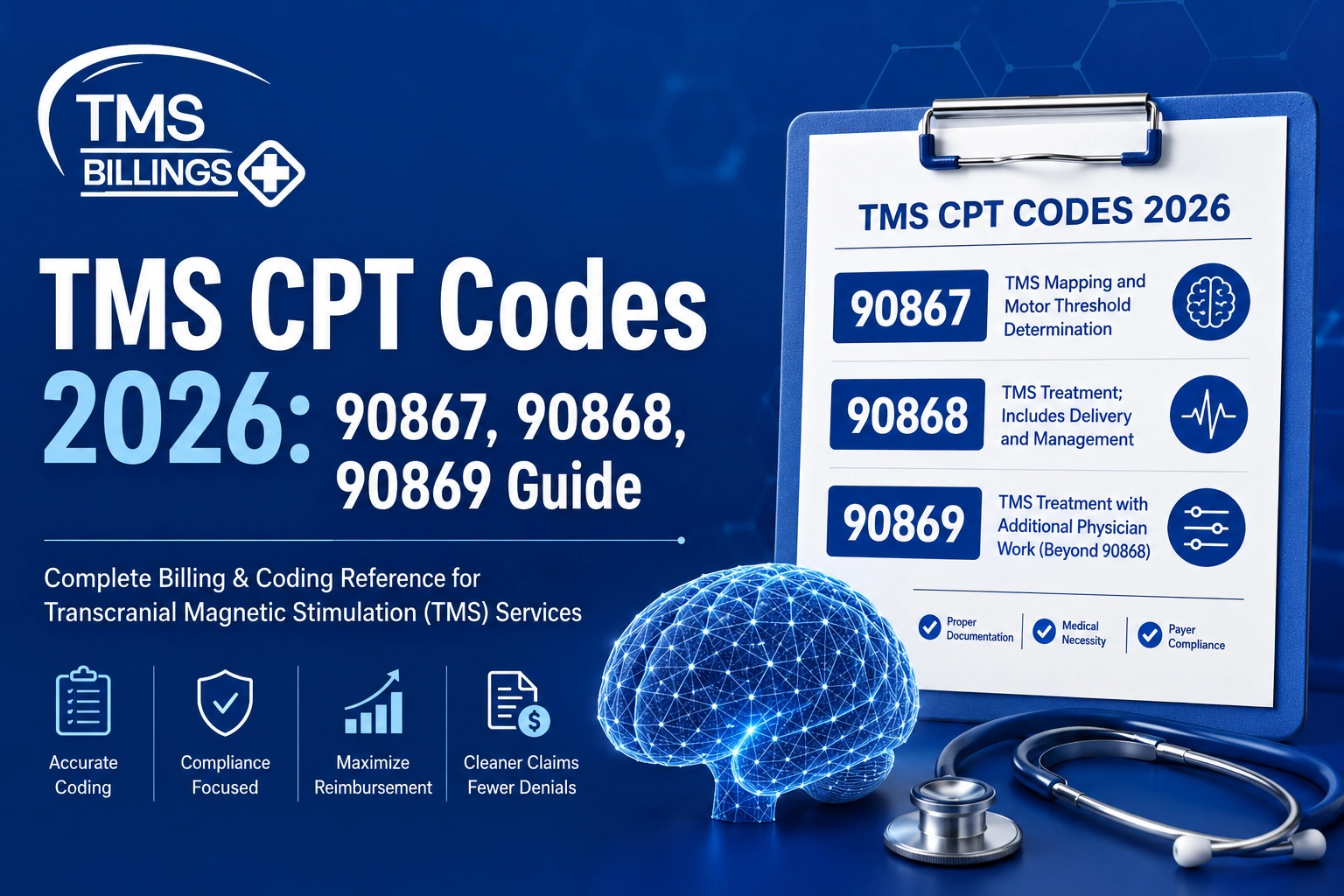
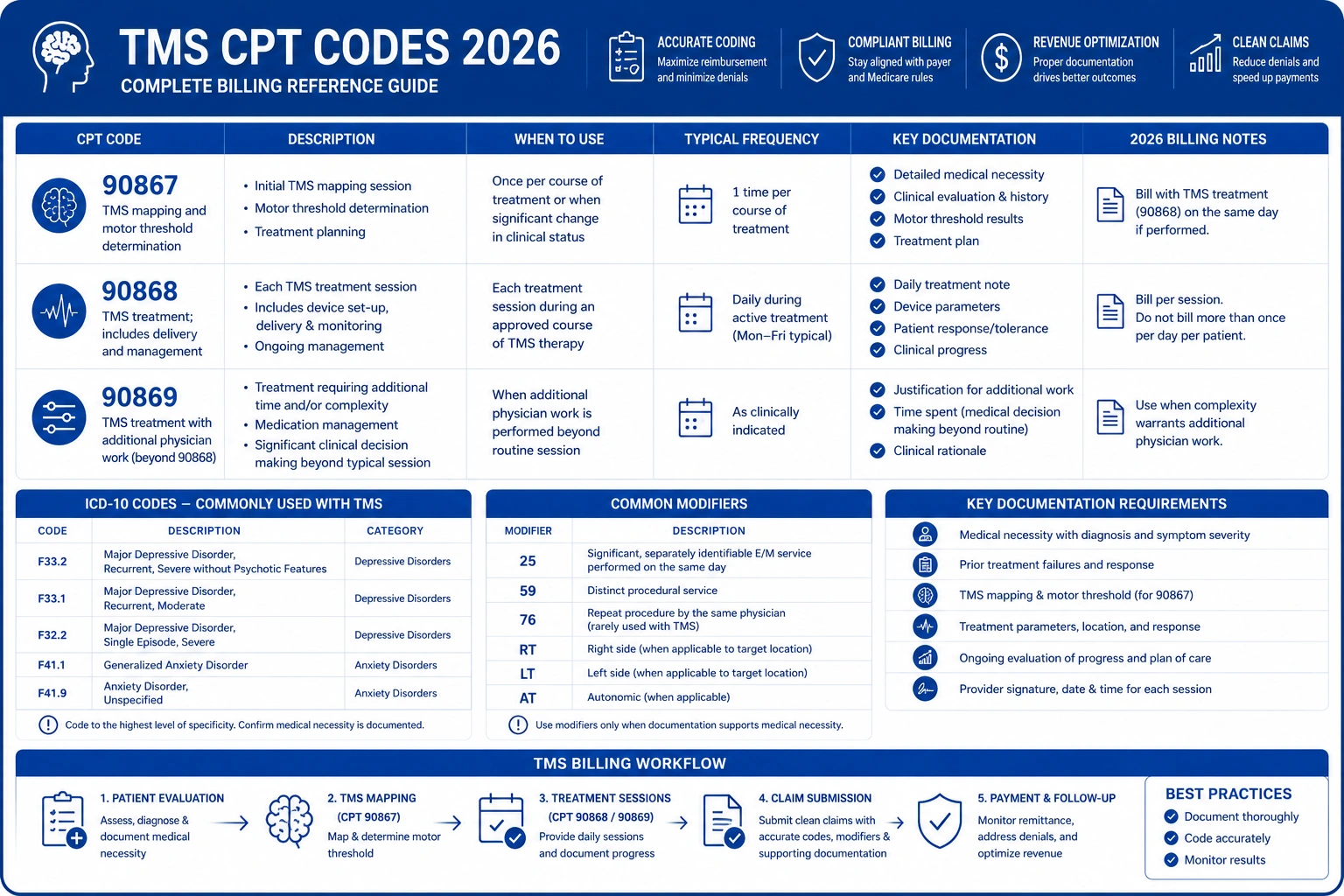
TMS CPT codes are the standardized procedure codes used to bill insurance for transcranial magnetic stimulation treatment. The three primary TMS CPT codes are 90867 (initial TMS session with cortical mapping and motor threshold determination), 90868 (subsequent TMS delivery and management), and 90869 (subsequent motor threshold re-determination). Using these codes correctly determines whether your claims are paid, denied, or flagged for audit.
TMS CPT codes 2026 operate within the same three-code framework established by the American Medical Association, but the billing rules, prior authorization requirements, and Local Coverage Determination policies around these codes have evolved. Staying current is not optional — it is a direct revenue imperative for any practice running a TMS program.
Why TMS CPT Code Accuracy Is a Revenue Priority for Every Practice
Transcranial magnetic stimulation billing consistently produces some of the highest denial rates in psychiatric practice. A single miscoded session in a 36-session treatment course can trigger a cascade of clawbacks, appeals, and authorization reviews that cost your team weeks of administrative rework — and your practice thousands in delayed or lost revenue.
What Changed in TMS Billing After Recent CMS and Payer Policy Shifts
CMS has continued refining its national and local coverage determinations for TMS, and commercial payers have followed with updated step therapy requirements and stricter prior authorization protocols. Many practices that built their billing workflows in 2022 or 2023 are now running processes that no longer match 2026 payer expectations. The gap between what your team submits and what payers require has widened — and that gap shows up directly on your denial report.
CMS and LCD Updates for TMS Coverage in 2026
CMS and LCD requirements for TMS coverage 2026 now demand more granular documentation of failed medication trials, more precise diagnosis code selection, and tighter alignment between the session type billed and the CPT code reported. Medicare’s local coverage determinations vary by MAC jurisdiction, and failure to follow the applicable LCD is the leading cause of Medicare TMS denials. Review the most current LCD and fee schedule updates for your region directly at CMS.gov.
Why Many Practices Are Still Leaving TMS Reimbursement on the Table
Most practices losing TMS revenue are not doing so through fraud or negligence. They are losing it through:
- Outdated code-to-diagnosis pairings that no longer match payer LCDs
- Incomplete prior authorization packets missing required step therapy elements
- Missed motor threshold re-determination billing opportunities (90869 billed as 90868)
- Billing staff who are unfamiliar with payer-specific step therapy requirements
- Credentialing gaps that delay payer enrollment for new TMS providers
The Hidden Revenue Risk of Incorrect TMS Procedure Codes
Every incorrectly billed TMS session costs your practice more than the denied claim itself. It triggers audit flags, delays subsequent payment processing, and creates documentation burden for your clinical team. TMS billing codes 2026 require precision at every step of the revenue cycle — from pre-authorization to final remittance posting. A single coding error in a high-value treatment course does not stay isolated; it affects claim adjudication downstream.
The Biggest Causes of TMS Billing Denials in 2026
Missing or Incomplete Prior Authorization for TMS Treatment
TMS prior authorization 2026 requirements vary significantly across commercial payers. Most require documented evidence of diagnosis, multiple failed medication trials, and a clinical justification letter — all submitted before the first session. Missing a single element results in a full-course denial. Payers do not send partial authorizations; an incomplete packet means zero sessions are covered until the authorization is corrected and re-approved.
Wrong ICD-10 Diagnosis Codes — Major Depressive Disorder vs. OCD
Diagnosis codes for major depressive disorder billing must align precisely with your payer’s coverage policy. Billing F33.2 (MDD, recurrent, severe without psychotic features) when the applicable LCD requires F33.1 (MDD, recurrent, moderate) — or the reverse — triggers an automatic denial. OCD TMS claims require F42.2 or F42.9 and must link to an FDA clearance pathway, not a standard depression LCD. These are not interchangeable.
Medicare LCD Confusion and Session Limit Errors
Medicare local coverage determination TMS policies limit the covered number of sessions per treatment course and require documentation that mirrors the pivotal clinical trials used to establish coverage. TMS session limits and treatment course billing must match the authorized session count exactly. Billing beyond the approved session range — even by one session — without an updated authorization is a guaranteed denial with clawback risk.
Documentation Gaps That Trigger Automatic Denials
Payers increasingly use automated claim scrubbing that flags notes missing required elements before a human reviewer ever sees the claim. If your session notes do not include motor threshold values, coil placement rationale, stimulation parameters, and patient response documentation, your claims will not survive an audit. This is not about effort — it is about template design and training.
Confusing Initial vs. Subsequent TMS Codes (90867 vs. 90868 vs. 90869)
This is the most common coding error in transcranial magnetic stimulation billing. CPT 90867 covers the initial TMS session with cortical mapping and motor threshold determination — it is billed once per treatment course. Every session after the first, unless it includes motor threshold re-determination, uses CPT 90868. Billing 90867 more than once in a single treatment course is a misuse that payers catch quickly through claim scrubbing.
Step Therapy and Failed Medication Trial Violations by Payer
Step therapy and failed medication trial documentation is required by virtually every commercial payer. If your prior authorization packet does not include clinical notes confirming trial and failure of the required number of antidepressant medications — at adequate doses and durations — your authorization will be denied before the first session is scheduled. Payer requirements range from two to six failed medication trials. Knowing which payer requires what is a fundamental billing competency.
The Complete TMS CPT Codes 2026 Billing Guide
CPT 90867 — Initial TMS Session With Cortical Mapping and Motor Threshold
CPT 90867 covers the initial TMS session with cortical mapping and TMS motor threshold determination billing. This code is used once per treatment course and encompasses:
- Cortical mapping to identify the optimal stimulation site (typically the left dorsolateral prefrontal cortex)
- Motor threshold determination to establish the safe and clinically therapeutic stimulation intensity
- Initial TMS treatment delivery
- Physician oversight and session management documentation
Per AMA CPT code guidelines, CPT 90867 cannot be billed for subsequent sessions, even if cortical mapping is informally revisited. If motor threshold must be formally re-determined mid-course, CPT 90869 applies — not 90867.
CPT 90868 — Subsequent TMS Delivery and Management
CPT 90868 is the core production code for a standard TMS treatment course. It covers:
- All subsequent TMS sessions following the initial cortical mapping session
- Ongoing clinical management of the TMS treatment protocol
- Documentation of patient response, parameter adjustments, and session tolerance
A standard 36-session treatment course typically generates one billing of 90867 and 35 billings of 90868. TMS reimbursement codes at the 90868 level form the majority of your TMS program revenue, making correct and consistent use of this code a direct financial priority.
CPT 90869 — Subsequent Motor Threshold Re-Determination
CPT 90869 is billed when motor threshold must be formally re-determined during an active treatment course — not at the start of treatment. This is appropriate when:
- The patient has experienced a significant medication change affecting cortical excitability
- There has been a clinically significant gap between sessions (typically 30+ days, though payer rules vary)
- Clinical indicators — reduced efficacy or patient-reported changes — suggest threshold drift
Billing 90867 instead of 90869 for a mid-course motor threshold re-check is one of the most common and costly TMS billing errors in practice. Payers detect it as a duplicate initial session code, deny it, and may flag the claim for further audit.
ICD-10 Codes That Support Medical Necessity for TMS
ICD-10 codes for treatment-resistant depression and OCD most commonly accepted for TMS coverage include:
| ICD-10 Code | Description | Common Payer Use |
|---|---|---|
| F33.2 | Major depressive disorder, recurrent, severe without psychotic features | Medicare and most commercial payers |
| F33.1 | Major depressive disorder, recurrent, moderate | Select commercial payers (verify LCD) |
| F32.2 | Major depressive disorder, single episode, severe | Some commercial payers |
| F42.2 | Obsessive-compulsive disorder | FDA-cleared TMS devices, select commercial payers |
| F42.9 | OCD, unspecified | Select commercial payers (verify separately) |
| F33.9 | Major depressive disorder, recurrent, unspecified | Rarely accepted — avoid unless payer-confirmed |
Always verify the accepted ICD-10 codes against the specific payer LCD or coverage policy before submitting. Diagnosis codes for major depressive disorder billing must match the severity level documented in the clinical note — a mismatch between the note and the claim is both a billing error and an audit trigger.
TMS Modifier Codes and Session Count Requirements
TMS modifier codes and session units are required by some payers to indicate:
- Modifier 26: Professional component only (when billing physician oversight separately from the technical delivery)
- Modifier TC: Technical component only (when billed by the facility separate from the supervising physician)
- Modifier 59: Distinct procedural service (used when multiple procedures are performed on the same day)
- Modifier GT: Via interactive audio/video telecommunication (telehealth-adjacent — rarely applicable for TMS)
Incorrect modifier use is a consistent denial trigger. Confirm modifier requirements payer by payer and update your billing grid whenever payer policies are revised.
How Much Revenue Is Your Practice Losing to TMS Billing Errors?
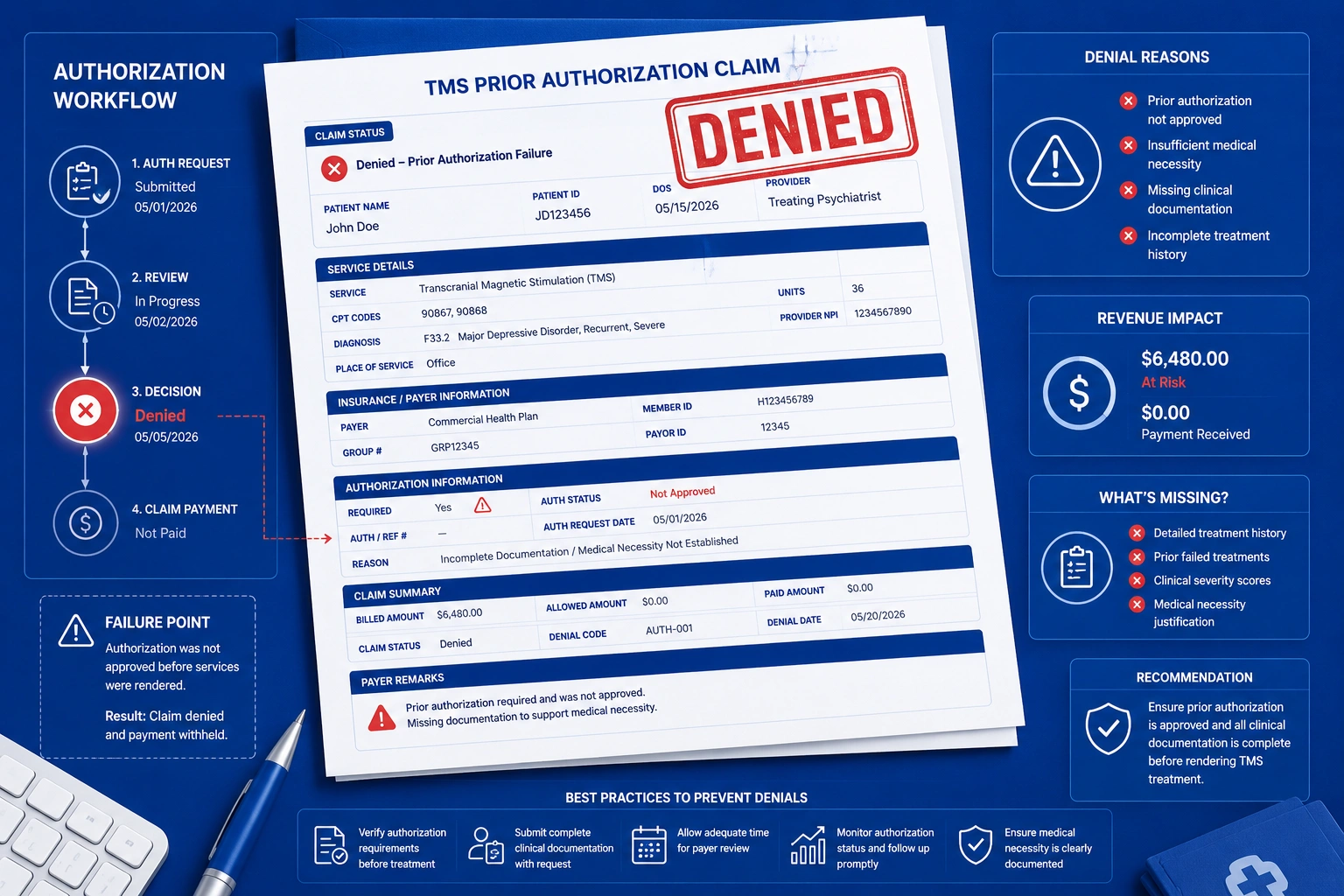
Example 1 — Wrong Diagnosis Code Leads to a Blanket Prior Auth Denial
A psychiatric practice submits a prior authorization for TMS using ICD-10 code F33.1 (MDD, recurrent, moderate). The commercial payer’s LCD only covers TMS for F33.2 (MDD, severe). The entire treatment course authorization is denied. The billing team submits an appeal, which takes three to four weeks to process. The patient’s treatment is delayed, the practice absorbs the administrative cost of rework, and the clinical relationship is damaged by a billing failure that had nothing to do with clinical care.
Revenue at risk: One 36-session TMS course at commercial rates of $150–$300 per session = $5,400–$10,800 per patient.
Example 2 — TMS Claims Denied for Incomplete Step Therapy Documentation
A practice’s prior authorization packet documents two failed antidepressants. The payer requires four failed trials with documentation of dose, duration, and reason for discontinuation. The authorization is denied outright. Step therapy and failed medication trial documentation is not a formality — it is a gatekeeping requirement that payers enforce at the PA stage. Without complete documentation for all required medications, no appeal will succeed until the documentation gap is closed.
Example 3 — Motor Threshold Re-Check Billed Incorrectly as an Initial Session
A patient returns for TMS after a 90-day treatment gap. The billing team submits CPT 90867, believing the re-start justifies an initial session code. The payer flags it as a duplicate 90867 submission within the same plan year. The claim is denied. The correct code was CPT 90869, which covers subsequent motor threshold re-determination during a resumed treatment course. Recovering this revenue requires a corrected claim, a detailed appeal, and a minimum 30-day delay in payment.
Medicare vs. Commercial Payer TMS Rules: A 2026 Comparison
What Medicare LCDs Require for TMS Coverage in 2026
Does Medicare cover TMS for depression in 2026? Yes — but under specific Medicare local coverage determination TMS conditions that vary by MAC jurisdiction. Standard Medicare LCD requirements include:
- Confirmed diagnosis of major depressive disorder (F33.2 or F32.2) with documented treatment resistance
- Failure of at least four antidepressant medication trials at adequate doses and durations
- No active substance use disorder diagnosis within the past six months
- No active or recent psychotic features documented in the clinical record
- Sessions delivered by or under the direct supervision of a licensed physician
- Documentation structure that mirrors the pivotal TMS clinical trial protocols
Visit CMS.gov to access your MAC’s applicable LCD and confirm the session limits, diagnosis requirements, and documentation standards specific to your billing region.
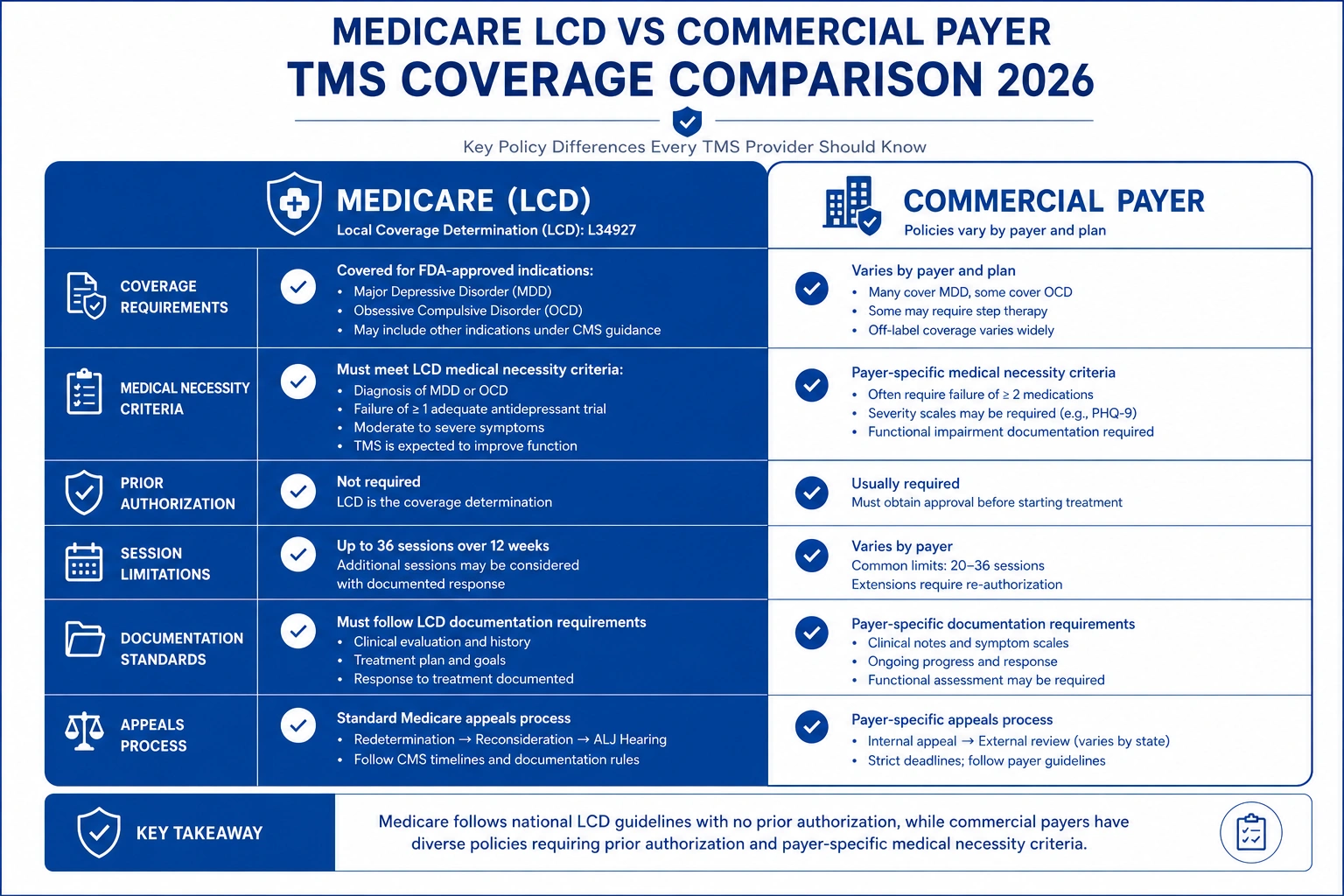
How Commercial Payers Differ From Medicare on TMS Coverage
| Coverage Factor | Medicare | Commercial Payers |
|---|---|---|
| Diagnosis Required | MDD, severe (F33.2 / F32.2) | MDD or OCD (varies by plan) |
| Failed Medication Trials | 4+ trials documented | 2–6 trials (varies by plan) |
| Session Limit Per Course | Per LCD (typically 36) | 20–36 (varies by plan) |
| Prior Authorization | Required | Always required |
| Physician Supervision | Direct supervision required | Varies by payer |
| OCD Coverage | Limited | Many plans cover (FDA-cleared TMS) |
| Re-treatment Authorization | New LCD review | New PA required (varies) |
| Bilateral TMS Coverage | Limited | Plan-specific |
Commercial payer TMS prior authorization requirements are typically more variable and more administratively burdensome than Medicare. Some commercial payers require a fresh prior authorization for every new treatment course — even for patients who have successfully completed TMS in the past and are seeking re-treatment.
Medicaid TMS Coverage Variation by State
Medicaid TMS coverage varies dramatically by state. As of 2026, approximately half of state Medicaid programs cover TMS for treatment-resistant depression under specific conditions. Coverage rules, ICD-10 acceptance, session limits, and prior authorization requirements differ significantly across state Medicaid agencies. Your billing team should maintain a current payer matrix specific to your state Medicaid program and review it quarterly for policy changes.
Documentation Requirements for TMS Claims
What Must Be in the Clinical Note to Support TMS Medical Necessity
Every TMS session note must include the following elements to survive payer audit:
- Patient diagnosis with ICD-10 code and corresponding severity specifier
- Motor threshold value at time of treatment (in percentage of maximum stimulator output)
- Coil placement — anatomical site and laterality
- Stimulation parameters: frequency (Hz), intensity (% MT), total pulses delivered, inter-train interval
- Session duration
- Patient response and tolerance documentation
- Physician attestation statement for supervised sessions (as required by payer)
- Any protocol adjustments and clinical rationale
Notes that are templated without individualization are among the most common triggers for payer audits and recoupment demands. Clinical documentation must reflect actual patient-specific care.
Prior Authorization Packets — What Payers Require for TMS in 2026
A complete TMS prior authorization 2026 packet typically requires all of the following:
- Completed payer-specific prior authorization request form
- Letter of medical necessity from the treating psychiatrist or supervising physician
- Failed medication trial documentation (drug name, dose, duration, reason for discontinuation) for each required trial
- Full psychiatric evaluation or intake assessment
- DSM-5 diagnosis confirmation with severity specifier
- PHQ-9 or equivalent validated depression rating scale scores (baseline and recent)
- Any prior TMS treatment history, outcomes, and re-treatment justification
The Clinical TMS Society publishes clinical practice guidelines that directly support the medical necessity argument in prior authorization letters. Referencing society-endorsed treatment protocols in your letter of medical necessity meaningfully strengthens your submission.
Avoiding Common Documentation Errors That Trigger Audits and Clawbacks
Most payer audits targeting TMS claims flag one or more of these specific errors:
- Missing motor threshold documentation in session notes
- Templated notes that do not reflect individualized clinical assessment
- Billed session dates that do not precisely match the dates documented in the clinical record
- Missing physician attestation from sessions that require direct supervision
- Discrepancies between the stimulation parameters in the clinical note and the parameters reflected in the billing data
- Session count that exceeds the authorized number without a supporting extension authorization
Audit-proof your documentation templates against this list before your next claims submission cycle. If you need help evaluating your current documentation practices, our Medical Coding Services team performs documentation compliance reviews specifically for TMS practices.
Strategies Every Practice Should Implement Right Now
Verify TMS Coverage and Prior Auth Requirements Before Scheduling
Check coverage eligibility, prior authorization requirements, and diagnosis code acceptance before scheduling the initial TMS consultation — not after. Do not assume approval based on a previous patient’s experience. Commercial payer TMS prior authorization policies change mid-year without notice, and a one-session difference in session limits can affect your entire treatment course.
Use the Correct Diagnosis and Session Code Combination for Each Payer
Maintain a payer-specific billing grid that maps:
- Accepted ICD-10 codes → by payer name and plan type
- Session code rules (90867 / 90868 / 90869) → by treatment phase and clinical event
- Modifier requirements → by payer and place of service
- Session limits and re-authorization thresholds → by payer
Update this grid whenever a payer issues a policy change notification or when a claim denial reveals a discrepancy.
Build a Standardized Prior Authorization Workflow for TMS
Create a checklist-based PA workflow that captures all required documentation at intake — before the patient is ever scheduled for treatment. This ensures that when the authorization is submitted, no elements are missing. Knowing how to bill TMS CPT codes in 2026 starts with a pre-session workflow that makes authorization approval the rule, not the exception.
Train Your Billing Staff on Payer-Specific TMS Codes and Step Therapy Rules
Step therapy and failed medication trial documentation requirements differ by payer and can change annually. Your billing staff should know which payers require two, three, or four failed medication trials; what documentation format each accepts; and how to escalate when a payer demands additional clinical evidence. Annual training updates aligned with payer policy cycles are not optional — they are a revenue protection measure.
Outsource TMS and Behavioral Health Billing to Specialists
If your practice does not have dedicated TMS billing expertise on staff, outsourcing to a specialist is the highest-ROI decision available to you. Generalist billing teams managing multiple specialties routinely miss TMS-specific payer nuances that specialist teams catch on first submission. Our Medical Billing Services are built specifically for psychiatric and TMS practices — and the difference shows up on your denial rate report within 90 days.
How Outsourced TMS Billing Protects Your Revenue
Proactive Prior Auth Denial Prevention for TMS Claims
This TMS billing guide 2026 can tell you what to do — but applying it consistently across a growing patient panel requires dedicated oversight. Specialist TMS billing teams proactively identify authorization gaps before submission, catching errors that in-house staff managing multiple specialties may not catch until a denial arrives three to five weeks later. Proactive prevention costs less than reactive rework — every time.
Faster, Fully Documented Appeals With Clinical Evidence
When denials do occur, specialist billing teams submit appeals supported by Clinical TMS Society clinical practice guidelines, payer-specific LCD language, and structured clinical evidence. Generic denial appeal letters fail. Evidence-backed appeals grounded in published clinical standards succeed at significantly higher rates and in less time.
Payer-Specific TMS Denial Tracking and Trend Reporting
Specialist billing partners use advanced Billing Reporting and Analytics tools to identify denial patterns by payer, CPT code, ICD-10 code, and billing period. When a payer begins denying a specific diagnosis code that was previously accepted, trend reporting surfaces that change within days — not quarters — enabling proactive correction before the pattern becomes a write-off.
How TMS Billings Helps Practices Maximize TMS Reimbursement

At TMS Billings, we specialize exclusively in psychiatric and TMS revenue cycle management. Our team manages TMS billing codes 2026 for practices ranging from single-provider TMS clinics to multi-site psychiatric groups treating hundreds of patients per month.
Our approach covers every dimension of TMS revenue protection:
- Pre-authorization review for every new TMS patient before session scheduling
- Real-time coding audits aligned with current LCD and commercial payer policies
- Provider credentialing through our Credentialing Services team to ensure your practice is enrolled correctly with every payer before your first TMS claim is submitted
- Denial management with documented appeal success rates above industry average
- Payer matrix updates delivered to your team as payer policies change throughout the year
- Session-level charge review to catch 90867/90868/90869 mismatches before submission
When you work with the TMS Billings team, your billing reflects the clinical precision your patients already experience in the treatment chair.
The Financial Cost of TMS Billing Errors in 2026
TMS reimbursement codes are among the highest-value procedure codes in psychiatric billing — and that makes coding errors disproportionately expensive. Here is what the current data shows:
- TMS treatment volume is growing year-over-year. As the evidence base for TMS in treatment-resistant depression strengthens and provider adoption accelerates, claim volume is rising — which means billing risk scales with it. The Clinical TMS Society has documented consistent year-over-year growth in TMS utilization across both academic and community psychiatric settings. More volume without updated billing workflows means compounding exposure.
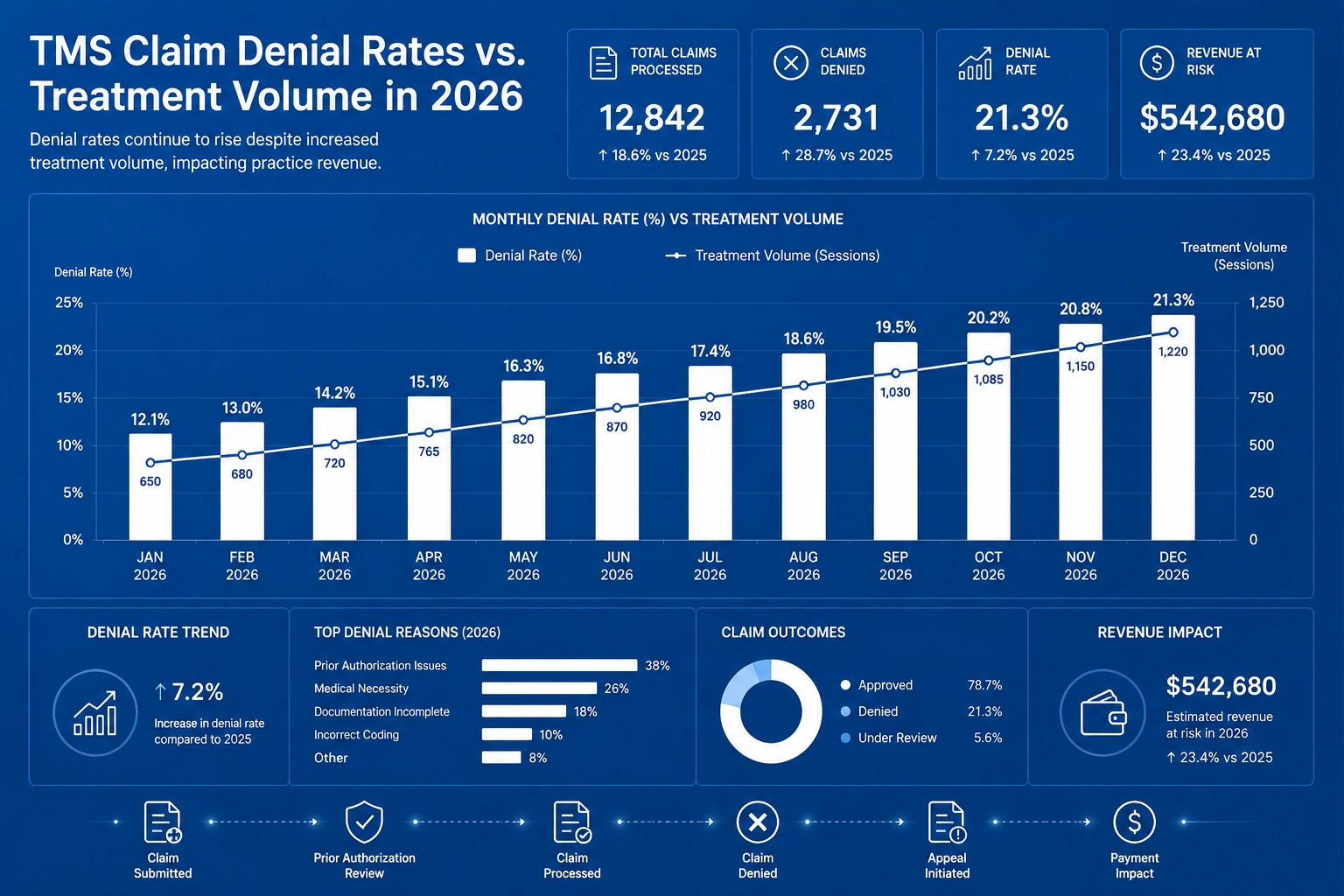
- Revenue at risk per denied 36-session course is significant. A single denied TMS treatment course at commercial payer rates of $150–$300 per session places $5,400–$10,800 at immediate risk. For a practice treating 20 TMS patients per quarter, a 10% first-pass denial rate translates to $10,800–$21,600 in quarterly write-offs — before accounting for the administrative cost of rework.
- The cost of reworking a denied TMS claim is substantial. Per AMA research on prior authorization burden, reworking a single denied claim costs providers an average of $25–$118 in administrative labor, with complex appeals — including TMS prior authorization disputes — consistently at the higher end of that range. Prior authorization burden also consumes physician time that could be directed to clinical care.
- The Medicare vs. commercial payer reimbursement gap is real. Medicare reimbursement per TMS session under the physician fee schedule is typically $30–$90 lower per session than contracted commercial payer rates. Practices that lose commercial authorizations and fall back to Medicare rates face significant per-course revenue compression — sometimes $1,000–$3,000 per patient per course.
- First-pass TMS claim success rates lag other psychiatric procedure types. Industry data indicates that TMS claims have a higher-than-average first-pass denial rate compared to other psychiatric procedures, driven primarily by prior authorization errors and incorrect diagnosis code selection. Moving first-pass rates from 70% toward 90%+ is achievable with specialist billing oversight — and every percentage point represents real revenue recovered.
Key Takeaways
- TMS CPT codes 2026 center on three codes: 90867 (initial session with cortical mapping and motor threshold determination), 90868 (subsequent delivery and management), and 90869 (subsequent motor threshold re-determination)
- CPT 90867 is billed once per treatment course — billing it again mid-course is a coding error that payers catch and deny automatically
- ICD-10 diagnosis codes must match payer-specific LCD requirements exactly — even minor mismatches between severity specifiers trigger denials
- Prior authorization is required by virtually all payers and must be submitted with complete step therapy and failed medication trial documentation before session one
- Medicare LCD rules and commercial payer rules differ significantly — your billing team needs a current, payer-specific billing grid
- Documentation quality determines claim survival — motor threshold values, stimulation parameters, and physician attestation are non-negotiable elements
- TMS billing codes 2026 require payer-specific expertise — generalist billing teams routinely miss nuances that specialist teams catch before submission
- Outsourcing to TMS billing specialists delivers measurable ROI through higher first-pass rates, fewer write-offs, and faster appeal resolution
Final Thoughts
TMS CPT codes 2026 — 90867, 90868, and 90869 — are not inherently complicated. The rules, however, are specific, payer-variable, and updated without warning. A single coding error in a 36-session treatment course can cost your practice thousands in denied revenue, weeks in rework, and significant strain on your patient relationship.
The practices protecting their TMS revenue in 2026 treat billing with the same precision they bring to clinical care. They verify before scheduling, document with intention, track denial trends, and invest in the billing expertise that protects a high-value treatment program.
If your TMS billing is producing denial rates above 5%, missing prior authorizations, or struggling with step therapy documentation, the solution is not more effort — it is the right expertise applied consistently. Contact the TMS Billings team today to schedule a complimentary revenue cycle review and find out exactly how much reimbursement your practice is leaving behind.