

The 2026 Medicare physician fee schedule is final — and the headline “pay increase” hides a much more complicated story for your practice. CMS published the CY2026 Physician Fee Schedule in November 2025, introducing dual conversion factors, a new efficiency adjustment to work RVUs, tightened site-of-service payment rules, and expanded MIPS Value Pathways requirements. If your Revenue Cycle Management Services strategy hasn’t been updated to reflect these changes, your reimbursements are already at risk.
Understanding exactly how the 2026 Medicare physician fee schedule affects your specialty and your billing workflows is the first step toward protecting your revenue this year.
What Is the 2026 Medicare Physician Fee Schedule?
The 2026 Medicare physician fee schedule is CMS’s annual payment framework that determines how much Medicare pays physicians for covered services. Updated each calendar year, it sets conversion factors, relative value units (RVUs), and billing policies that directly control reimbursement for every CPT code billed to Medicare — effective January 1, 2026.
Why the 2026 Medicare Physician Fee Schedule Is a Revenue Priority for Every Practice
The CMS 2026 final rule touches every corner of how you bill Medicare — from the conversion factor applied to each CPT code to how work RVUs are calculated for time-based and non-time-based services. Asking how does the 2026 Medicare physician fee schedule affect my practice is the right starting question. The answers depend on your specialty, your service setting, and whether your practice participates in a qualifying Alternative Payment Model.
What Changed in the 2026 Medicare Physician Fee Schedule: Proposed vs. Final Rule
CMS released its proposed rule in July 2025. The final rule — published in the Federal Register in November 2025 — retained most major proposals but made targeted adjustments in response to physician commentary and specialty society advocacy. Key refinements from proposed to final included:
- Modified methodology for the efficiency adjustment applied to non-time-based services
- Adjusted allocations for indirect practice expense RVUs
- Clarified standards for telehealth and virtual direct supervision
- Expanded MIPS Value Pathways 2026 participation tracks for small and rural practices
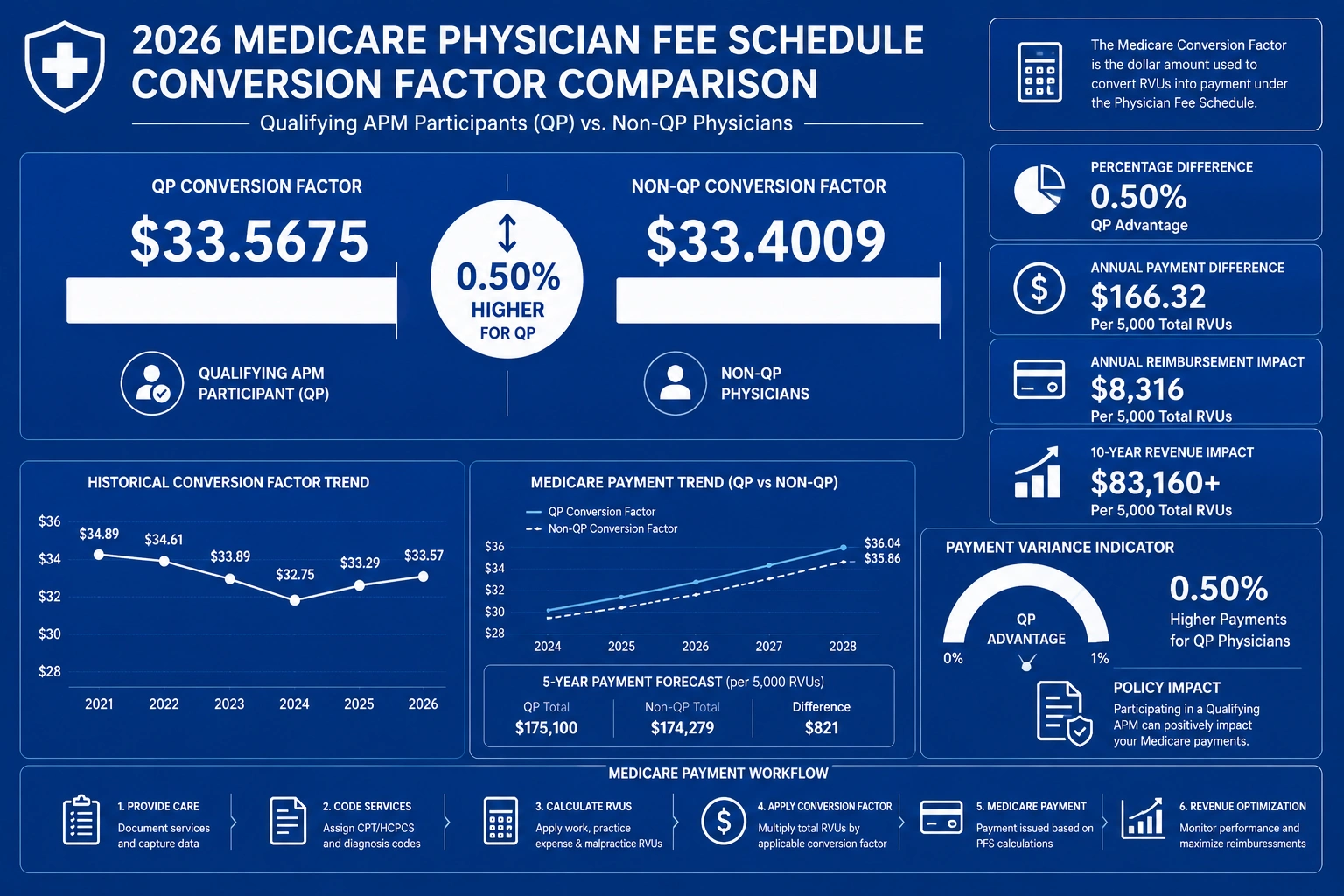
The Two New Conversion Factors: Qualifying APM vs. Non-QP
The most structurally significant change in the physician fee schedule changes 2026 is the formal split of the Medicare conversion factor 2026 into two distinct rates:
- Qualifying APM Conversion Factor: $33.5675
- Non-QP Conversion Factor: $33.4009
The qualifying APM conversion factor vs non-QP conversion factor gap is approximately $0.17 per RVU — a meaningful incentive over hundreds of monthly claims. Practices in qualifying Alternative Payment Models receive the higher rate as a reward for value-based care participation. Every other eligible clinician is paid at $33.4009.
Why a “Pay Increase” Headline Doesn’t Guarantee More Revenue
Two offsetting mechanisms reduce the actual dollars your practice collects — even with higher conversion factors:
- Efficiency adjustment to work RVUs — reduces reimbursement for non-time-based procedural services
- Site-of-service payment differential — redistributes payments away from facility settings
Combined, these adjustments mean many specialties face a net Medicare pay cut 2026 despite the higher headline conversion factor. Knowing which category your services fall into is essential before assuming you’ll see more revenue this year.
The Biggest Changes in the 2026 Medicare Physician Fee Schedule Final Rule
What changed in the CMS 2026 physician fee schedule final rule extends well beyond the conversion factor headline. Here are the policy changes with the greatest financial impact on your bottom line.
New Dual Conversion Factors ($33.5675 vs. $33.4009)
CMS set two separate conversion factors effective January 1, 2026. Here is the $33.5675 and $33.4009 conversion factor explained in practical terms: the higher rate applies exclusively to QP participants in qualifying APMs; the standard $33.4009 applies to all other eligible clinicians. Most physicians billing traditional Medicare fee-for-service use $33.4009.
How to calculate your expected reimbursement for any CPT code:
Payment = (Work RVU + Practice Expense RVU + Malpractice RVU) × Geographic Practice Cost Index × Conversion Factor
A service with a total of 3.0 RVUs pays a non-QP physician $33.4009 × 3.0 = $100.20 — and a QP physician $33.5675 × 3.0 = $100.70.
The Efficiency Adjustment to Work RVUs
CMS introduced the Medicare efficiency adjustment to work RVUs as a mechanism to account for assumed economies of scale in high-volume, non-time-based services. The adjustment applies a modest reduction to the work RVU component of certain procedures, reflecting CMS’s position that repetitive, high-volume services become incrementally less resource-intensive per unit over time.
This adjustment disproportionately affects high-volume procedural specialists who bill primarily for non-time-based services — including orthopedic surgeons, gastroenterologists, and ophthalmologists. Time-based services are not subject to the same adjustment.
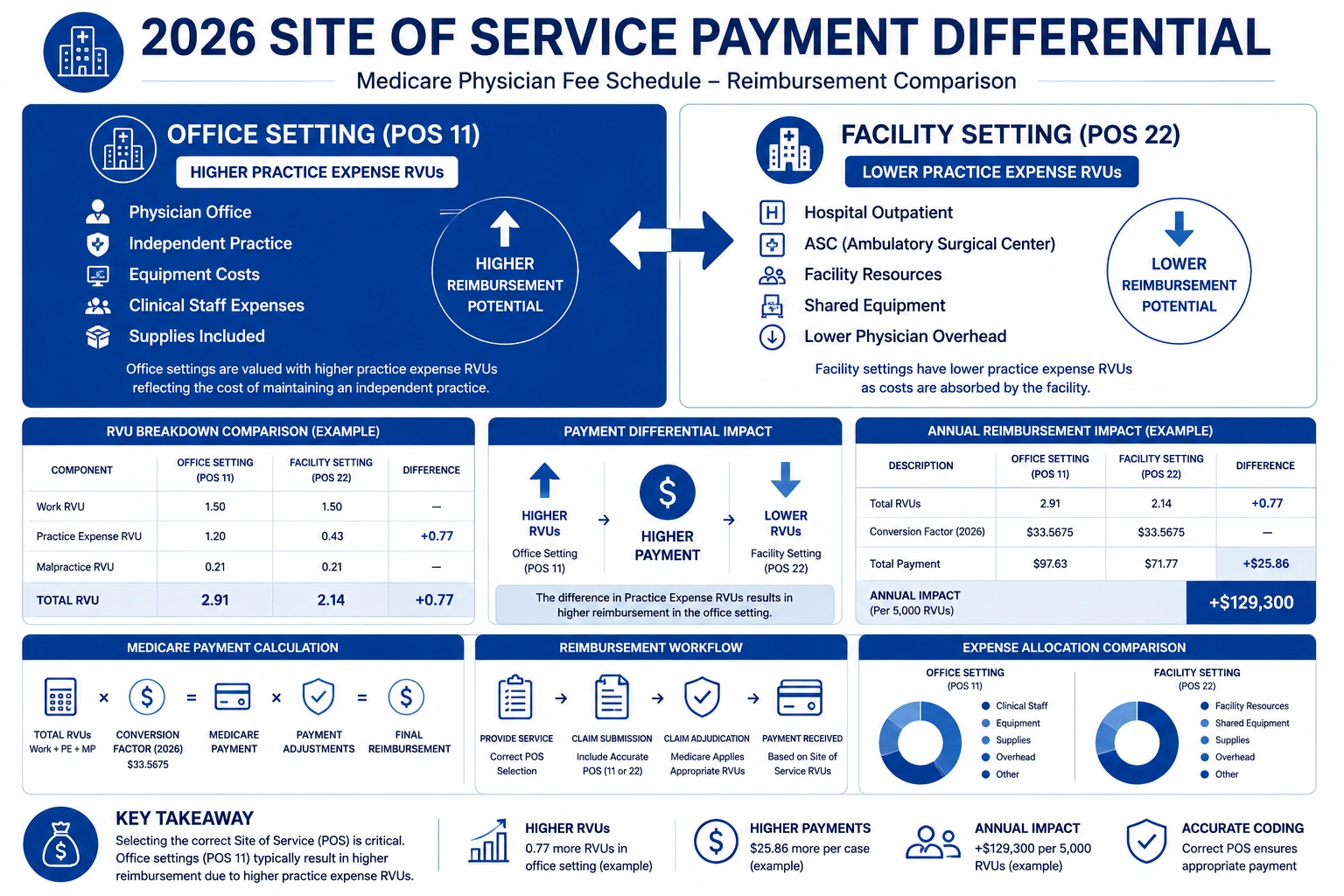
Site-of-Service Payment Differential (Office vs. Facility)
The site of service payment differential 2026 is one of the most financially consequential changes for procedural specialties. When a service is performed in a hospital outpatient department (HOPD) or ambulatory surgery center (ASC), Medicare pays the physician a reduced fee because the facility receives a separate facility fee. The physician’s relative value units and indirect practice expense components are lower in the facility setting.
In 2026, CMS narrowed the RVU gap between office and facility payment rates. Practices that shifted procedures to hospital outpatient settings lose more per procedure than prior-year models predicted. How does the site of service payment differential affect specialists? Facility-based cardiologists, orthopedic surgeons, and procedural specialists absorb the largest revenue hit.
Telehealth and Virtual Supervision Rule Changes
CMS extended several telehealth flexibilities that were set to expire, while also codifying updated standards for telehealth virtual direct supervision Medicare 2026. Under the new rule, supervising physicians may fulfill direct supervision requirements via two-way real-time audio-video technology without being physically present in the office suite. Billing updates your team must implement:
- New codes added to the permanent telehealth services list
- Updated place-of-service requirements: POS 10 (patient’s home) and POS 02 (other telehealth locations)
- Revised modifier requirements for synchronous audio-video visits (modifiers 95 and GT)
- New documentation standards for virtual supervision encounters
MIPS, MIPS Value Pathways, and Quality Payment Program Updates
The 2026 Quality Payment Program cycle expands MIPS Value Pathways 2026, offering specialty-specific reporting frameworks that require fewer measures but with stronger clinical relevance. Notable changes include:
- Raised performance thresholds for exceptional performance bonuses
- Updated cost category weighting in the composite MIPS score
- New small and rural practice reporting options with reduced administrative burden
- Expanded MVP tracks covering additional specialties and care settings
The American Medical Association has published specialty-level breakdowns of these QPP changes and their financial implications for practices navigating the transition to MVPs.
The New Mandatory Ambulatory Specialty Model (2027 Preview)
CMS’s Innovation Center finalized the framework for the Ambulatory Specialty Model heart failure and low back pain program, which launches in 2027 for practices in targeted geographies. This model provides bundled episode-based payments for two high-cost, high-volume conditions. While not yet mandatory in 2026, practices in eligible areas must begin preparing now — evaluating their episode-of-care data, care coordination infrastructure, and technology readiness.
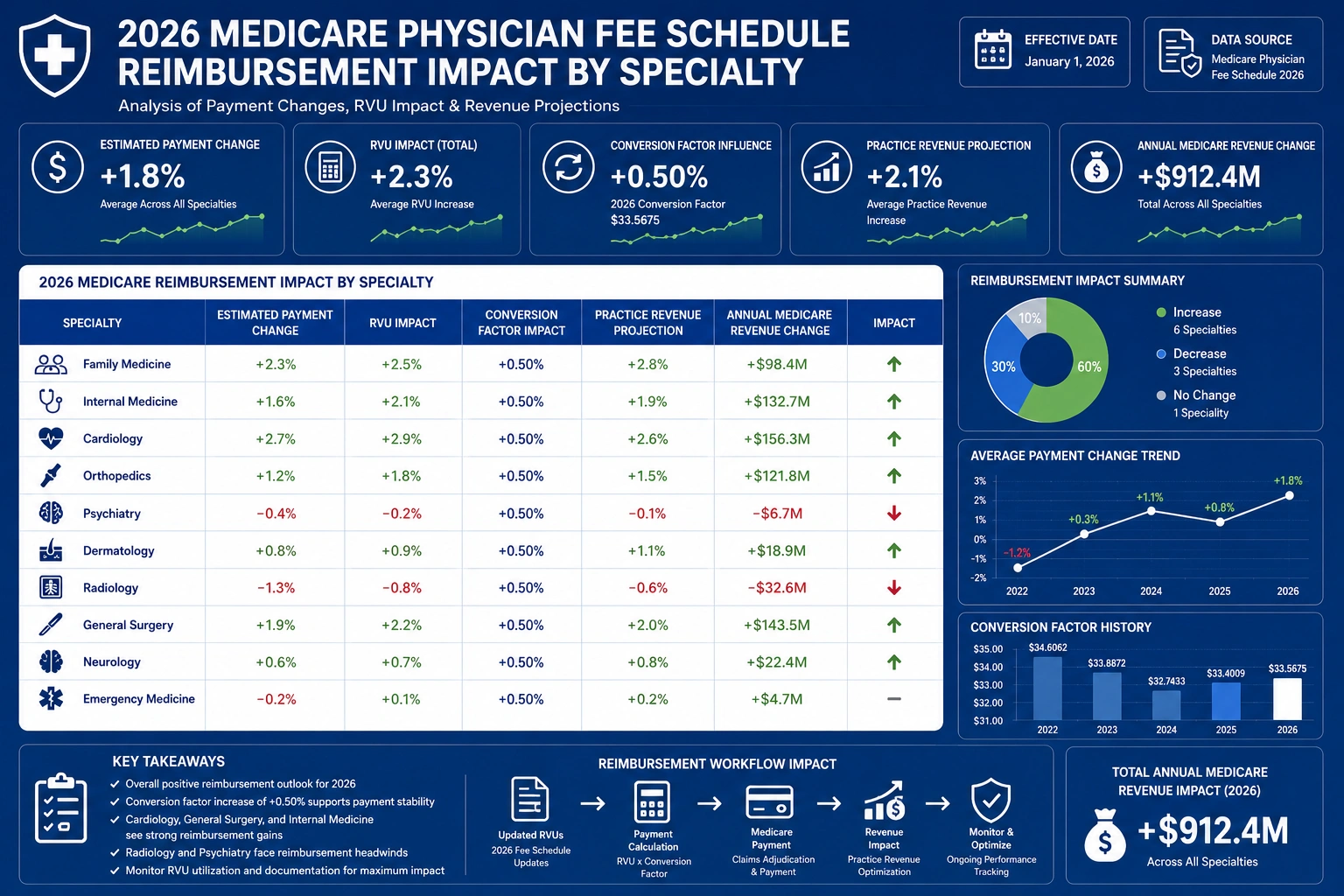
How the 2026 Physician Fee Schedule Affects Reimbursement by Specialty
Specialties Performing Mostly in Office Settings
Office-based specialties — primary care, family medicine, dermatology, psychiatry, and outpatient internal medicine — generally fare better under the 2026 rule. Higher non-facility practice expense allocations and limited exposure to the site-of-service differential mean these practices see modest revenue stabilization or modest gains from the higher conversion factor.
Specialties Performing Mostly in Facility/Hospital Settings
Facility-based specialties absorb the combined weight of the efficiency adjustment and the 2026 site-of-service payment differential. Surgical specialists, hospital-based proceduralists, and outpatient procedure centers are most at risk of a net revenue decline — regardless of the headline conversion factor increase.
Example: Cardiology, Orthopedics, and Procedural Specialties
A cardiologist performing echocardiograms in a hospital outpatient department may see per-unit reimbursement fall due to narrowed site-of-service RVU differentials. An orthopedic surgeon performing arthroscopic knee procedures faces both the efficiency adjustment on non-time-based work RVUs and reduced non-facility PE allocation. The Medicare reimbursement changes 2026 compound across high-volume practices with facility-heavy service mixes.
2026 Specialty Impact Comparison Table
| Specialty | Service Setting | CF Applied | Efficiency Adj. | Site-of-Service Impact | Estimated Net Change |
|---|---|---|---|---|---|
| Primary Care / Family Medicine | Office | $33.4009 | Minimal (time-based) | None | +2% to +3% |
| Psychiatry / Behavioral Health | Office | $33.4009 | Minimal (time-based) | None | +2% to +3% |
| Orthopedic Surgery | Facility / ASC | $33.4009 | Applies | Negative | −1% to −3% |
| Interventional Cardiology | Facility / HOPD | $33.4009 | Applies | Negative | −2% to −3% |
| Gastroenterology | Facility / ASC | $33.4009 | Applies | Negative | −1% to −3% |
| Qualifying APM Participant | Any | $33.5675 | Varies | Varies | +0.5% vs. Non-QP |
Estimated ranges based on CMS impact tables and RVU redistribution modeling. Individual practice impact varies by payer mix, CPT code volume, and geographic location.
How Much Could Your Practice Gain or Lose Under the 2026 Rule?
Example 1 — Office-Based Primary Care Practice
A primary care practice billing 500 E&M visits per month at an average of 1.5 total RVUs each:
- CY2025 payment per visit: 1.5 × $32.3465 ≈ $48.52
- CY2026 non-QP payment per visit: 1.5 × $33.4009 ≈ $50.10
- Gain per visit: ~$1.58 | Monthly gain: ~$790 | Annual gain: ~$9,480
For this practice type, the physician fee schedule changes 2026 represent a genuine revenue improvement — assuming documentation and coding accuracy are maintained.
Example 2 — Facility-Based Procedural Specialist
A gastroenterologist performing 200 colonoscopies per month in a hospital outpatient setting:
- Efficiency adjustment reduces non-time-based work RVUs by an estimated 0.5%–1.0%
- Narrowed site-of-service differential further compresses per-procedure non-facility PE
- Net result: 2%–4% reimbursement reduction per procedure versus prior-year projections
This is a real Medicare pay cut 2026 — delivered quietly, through policy mechanics rather than a headline rate change.
Example 3 — Practice Participating in a Qualifying APM
A cardiology group participating in a qualifying ACO applies the $33.5675 QP rate:
- Per-RVU advantage over non-QP peers: ~$0.17
- At 1,000 monthly RVUs billed to Medicare: ~$170/month advantage
- Annualized advantage from CF differential alone: ~$2,040
APM participation continues to carry a compounding financial advantage — before any shared savings distributions are factored in.
Medicare vs. Commercial Payer Rates: How the Gap Is Shifting in 2026
What the New Conversion Factors Mean for Medicare Patients
The new Medicare conversion factor 2026 values set the floor for your Medicare revenue. But the conversion factor alone doesn’t capture total revenue impact when the efficiency adjustment and site-of-service differential are layered on top. Practices with high Medicare patient volumes feel these mechanics most acutely — and must model their full CPT code portfolio, not just their highest-volume codes.
Why Commercial Contract Benchmarking Matters More Than Ever
Commercial payers frequently benchmark their rates to Medicare as a percentage. When Medicare rates shift — even modestly — contracts tied to Medicare percentages shift too. 2026 is the year to audit every commercial contract due for renewal. Your Medical Billing Services team should flag any contract benchmarked to a prior-year Medicare fee schedule and flag it for renegotiation. Use the updated relative value units and indirect practice expense figures from the CMS 2026 final rule as your negotiating baseline. Any contract pegged below 115%–120% of Medicare may be materially undervaluing your services.
Documentation and Coding Adjustments Practices Need to Make
Your Medical Coding Services team needs to understand how the 2026 rule changes documentation requirements — not just conversion factors. Errors at the coding level amplify payment shortfalls that the fee schedule already creates.
Coding for Time-Based vs. Non-Time-Based Services
Because the efficiency adjustment applies specifically to non-time-based services, correctly identifying and documenting time-based encounters carries greater financial weight in 2026. Prolonged E&M visits, critical care, and certain counseling services should be coded using appropriate time-based codes with thorough time documentation. Time-based coding sidesteps the efficiency adjustment and preserves higher reimbursement for complex patient encounters.
Avoiding RVU and Site-of-Service Coding Errors That Compound the Cuts
A place-of-service coding error — billing non-facility rates for a hospital-based service — triggers the wrong RVU set, creates overpayment risk, and invites payer audits. Auditing POS codes against actual service locations is non-negotiable in 2026. Given how the site of service payment differential 2026 works, a single systematic POS error across high-volume claims compounds quickly into significant over- or underpayments.
Telehealth Billing Updates to Implement Now
Staff must be trained on updated billing requirements for telehealth encounters, including:
- POS 10 for services delivered to patients in their home
- POS 02 for other telehealth service locations
- Modifier 95 for real-time synchronous audio-video visits
- Modifier GT for Medicare telehealth services when applicable
- Updated documentation requirements for telehealth virtual direct supervision Medicare 2026 encounters
Strategies Every Practice Should Implement Right Now
Run a Specialty-Specific Impact Analysis on Your Top CPT Codes
Pull your top 25–30 CPT codes by claim volume. Apply the new CY2026 RVU values and the appropriate conversion factor — $33.5675 or $33.4009. Calculate the dollar-per-code delta against CY2025 payments. This analysis tells you exactly where your revenue is at risk and which service lines need the most attention.
Renegotiate Commercial Payer Contracts Using the New Benchmarks
Use the updated CMS.gov fee schedule as negotiating leverage for every commercial contract under review. Contracts benchmarked to outdated Medicare rates are costing you money. If a payer’s contract references a prior-year conversion factor, 2026 is the time to correct it.
Audit Site-of-Service Coding for Accuracy
Conduct a retrospective audit of Q4 2025 claims. Identify any place-of-service mismatches between the code billed and the actual location of service. Accurate Credentialing Services and payer enrollment records ensure your billing team always has the right service location on file before claims go out.
Train Billing Staff on the New Conversion Factor Rules
Your team needs clear, documented guidance on:
- Which conversion factor applies to your practice ($33.5675 QP or $33.4009 non-QP)
- How the efficiency adjustment changes work RVU calculations for specific CPT codes
- How to identify and correctly code time-based vs. non-time-based services
- Updated telehealth billing codes, modifiers, and documentation requirements
Outsource Revenue Cycle Management to Stay Ahead of CMS Rule Changes
For many practices, the complexity of the CMS 2026 final rule makes in-house billing increasingly expensive and risky. Annual rule cycles require constant retraining, workflow updates, and real-time monitoring — resources that stretch most in-house teams. Outsourcing to an RCM partner with dedicated CMS rule expertise protects revenue without adding internal headcount or overhead.
How Outsourced Billing Protects Your Revenue Under the New Fee Schedule
Proactive Reimbursement Monitoring by CPT Code
An experienced RCM partner tracks reimbursement per CPT code every month, flagging unexpected declines that signal coding errors, payer underpayments, or misapplication of the new rule. Your Billing Reporting and Analytics dashboard should surface these alerts automatically — not six months after the fact.
Faster Adaptation to CMS Rule Changes
When CMS issues a correction notice or interim guidance mid-year, your billing workflows need to update within days. Outsourced RCM teams focused exclusively on Medicare billing policy can adapt faster than in-house staff managing dozens of competing priorities simultaneously.
Specialty-Specific Revenue Cycle Reporting
Generic billing reports miss specialty nuance. The right RCM partner delivers reporting segmented by CPT code, service location, and payer — giving practice owners and CFOs the data needed to make informed decisions about patient mix, service line strategy, and contract renegotiation timing.
How TMS Billings Helps Practices Maximize Reimbursement in 2026

At TMS Billings, our revenue cycle management team monitors every CMS rule cycle — including every change in the 2026 Medicare physician fee schedule — so your practice doesn’t have to carry that burden alone. We deliver:
- Pre-rule specialty impact analyses — before the new payment rates take effect
- CPT code-level reimbursement tracking — monthly, with anomaly alerts
- Commercial payer contract benchmarking — using updated Medicare fee schedule data as the baseline
- Billing workflow updates — aligned with every change in the CMS 2026 final rule
- Full MIPS, QPP, and telehealth compliance monitoring — across the entire calendar year
Our clients don’t discover rate problems months after the fact. They prevent them.
The Financial Impact of the 2026 Fee Schedule
The following data points frame the real financial stakes of the Medicare reimbursement changes 2026 — drawn from CMS.gov, the Federal Register, and AMA analysis:
1. Conversion Factor Year-Over-Year Change The non-QP Medicare conversion factor 2026 rose from $32.3465 (CY2025) to $33.4009 — an increase of approximately 3.3%. QP participants receive $33.5675, a gain of approximately 3.8%. Both rates represent the largest single-year CF increases in recent memory, though offsetting adjustments limit the real-world revenue impact.
2. Efficiency Adjustment Impact on Procedural Work RVUs CMS’s Medicare efficiency adjustment to work RVUs is estimated to reduce effective reimbursement per code by 0.5%–1.5% for non-time-based procedural services, with the largest impact falling on high-volume facility-based specialists. This offset is not reflected in headline conversion factor announcements.
3. Specialty-Level Impact Range Per CMS’s own impact tables published with the final rule, specialty-level reimbursement changes range from approximately +3% for office-based primary care and outpatient behavioral health specialties to −3% or lower for interventional cardiology, orthopedic surgery, and other high-volume facility-based procedural specialties. The Medicare Economic Index (MEI) productivity adjustment further narrows real purchasing power gains for specialties with nominally positive impact.
4. Skin Substitute Payment Policy Savings CMS finalized significant changes to the skin substitute payment policy, removing a large category of products from the average sales price-based methodology. These changes are projected to redistribute hundreds of millions of dollars annually within the Medicare system — reducing reimbursement for high-cost skin substitute-dependent procedures while preserving payment for lower-cost alternatives.
5. How the Headline CF Increase Is Offset While the non-QP CF increased by approximately 3.3%, the efficiency adjustment to non-time-based work RVUs offsets a meaningful share of that gain for procedural specialties. When combined with the tightened site-of-service payment differential 2026, many facility-based procedural practices are projected to see a flat or negative net revenue change from Medicare — despite the headline improvement. The Medicare Economic Index (MEI) productivity adjustment limits the real value of the conversion factor increase when adjusted for inflation in practice operating costs.
Key Takeaways
- The 2026 Medicare physician fee schedule introduces two conversion factors: $33.5675 (QP participants) and $33.4009 (all other eligible clinicians)
- A headline CF increase does not guarantee net revenue growth — the efficiency adjustment and site-of-service differential offset gains for many specialties
- Facility-based procedural specialties — cardiology, orthopedics, gastroenterology — face the largest reimbursement risk in 2026
- MIPS Value Pathways 2026 expand specialty-specific reporting options but raise performance thresholds
- Telehealth billing rules are updated and must be implemented immediately across all affected service lines
- The Ambulatory Specialty Model heart failure and low back pain program launches in 2027 — preparation begins now
- The One Big Beautiful Bill Act Medicare physician pay increase, if enacted, could modify some of these impacts; practices should monitor legislative developments closely
- Commercial contract renegotiation is essential whenever CMS updates the Medicare fee schedule
Final Thoughts
The 2026 Medicare physician fee schedule is complex — and the gap between the headline and the reality is wide enough to cost your practice tens of thousands of dollars per year if your billing strategy doesn’t account for every change. The efficiency adjustment, dual conversion factors, site-of-service differential, and updated telehealth rules interact in ways that require specialty-specific analysis, not generic billing assumptions.
If you’re ready to understand exactly how the Medicare reimbursement changes 2026 affect your CPT codes, service mix, and payer contracts, TMS Billings is ready to help. Contact us today for a complimentary practice impact analysis and get a clear picture of what the 2026 rule means for your revenue.


