

A/R Aging Report in Medical Billing: What It Is and How to Use It
Every dollar your practice earns starts as a claim—and every claim that goes unworked becomes revenue at risk. The A/R aging report is the single most important tool your billing team has for knowing exactly where that revenue stands. If your practice is relying on our AR recovery services or managing collections in-house, understanding how to read and act on your A/R aging report is non-negotiable for protecting cash flow.
This guide covers everything: what an aging report is, how to read it bucket by bucket, what the benchmarks mean for your specialty, and the step-by-step process for reducing high A/R aging before it turns into a write-off.
What Is an A/R Aging Report?
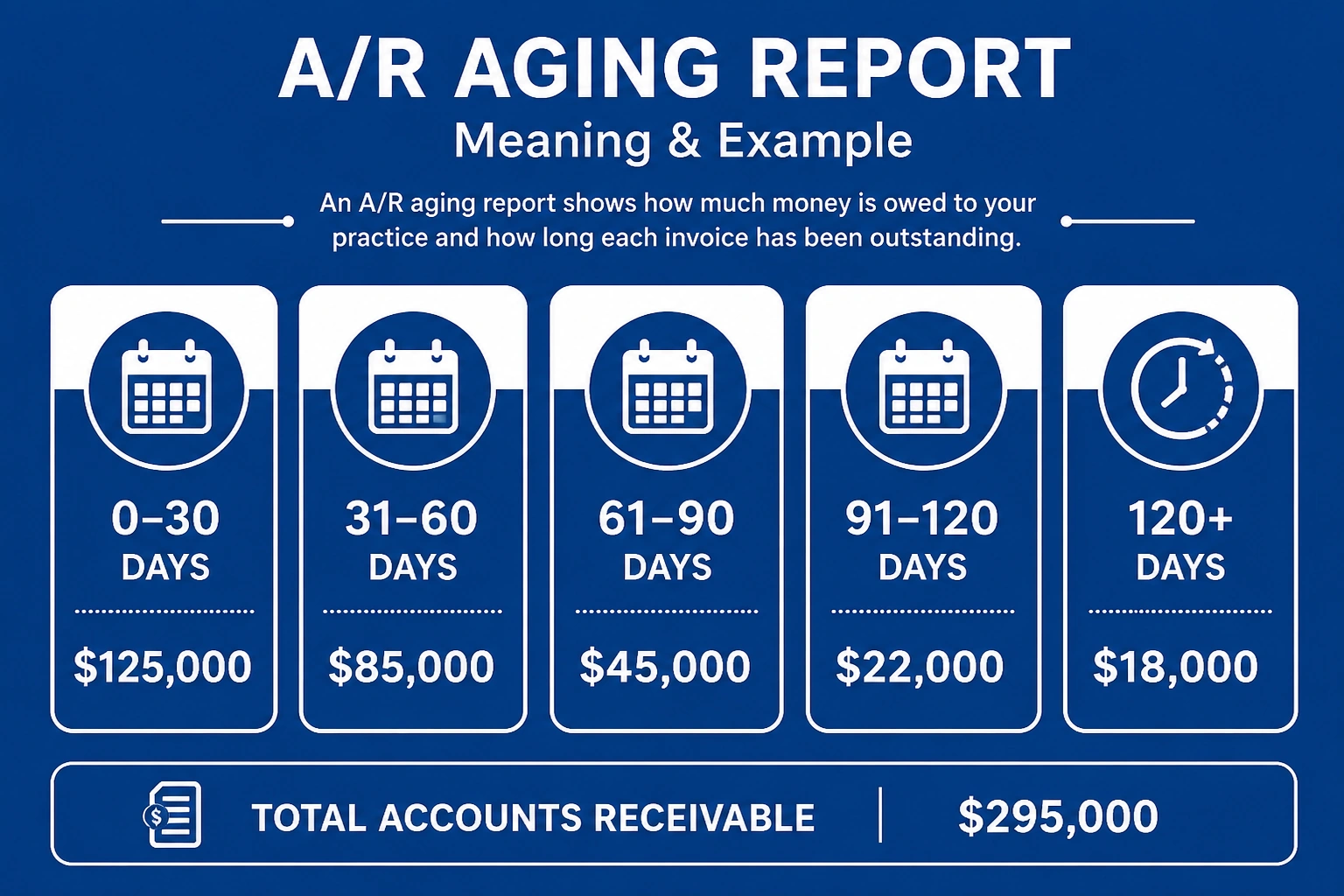
Featured Snippet: An A/R aging report is a financial tool that categorizes outstanding claims by how long they have been unpaid—typically in 0–30, 31–60, 61–90, 91–120, and 120+ day buckets. It gives billing teams a real-time snapshot of overdue payments and helps prioritize follow-up to protect practice revenue.
The A/R aging report is not just a list of unpaid claims. It is a prioritization tool. It tells your billing team exactly where revenue is stalled—and, critically, how urgently they need to act. A claim sitting in the 0–30 day bucket is in normal adjudication. A claim in the 91–120 day bucket is approaching the edge of collectability. A claim past 120 days is likely heading toward a write-off without immediate escalation.
Your accounts receivable (AR) balance is the total amount owed to your practice by payers and patients. The A/R aging report breaks that balance down by age, giving you visibility that a simple total cannot provide.
How to Read an A/R Aging Report
Reading an accounts receivable aging report correctly is the foundation of effective billing follow-up. Each row represents a payer or patient account, and each column represents a time bucket. The dollar amount in each cell tells you how much is outstanding in that age range.
A healthy practice should have 65–75% of total A/R sitting in the 0–30 day bucket, with under 15% combined in the 91+ day columns. When you see that ratio flip—large concentrations in the older buckets—your billing team has a follow-up problem that needs immediate attention.
Understanding Aging Buckets: 0–30, 31–60, 61–90, 91–120, and 120+ Days
The AR aging buckets are the columns of your A/R aging report. Here is what each one signals:
0–30 Days: Claims in normal adjudication. Standard payer processing runs 14–30 days. No action needed unless the claim is flagged as rejected.
31–60 Days: Claims that should be nearing payment. If a payer hasn’t responded by day 45, initiate a status check. Work any ERA/EOB discrepancies now.
61–90 Days: This bucket demands attention. File an appeal or resubmit any denied claims. Check for CARC codes (such as CO-45 or CO-97, defined by X12) that indicate contractual adjustments or duplicate claim issues.
91–120 Days: High-priority escalation zone. These outstanding claims have a falling collection probability—once a claim crosses 90 days, recovery rates drop below 50%. Escalate to a supervisor or payer provider relations contact.
120+ Days: These are critical. Collection rates for claims over 120 days fall below 50% across most payer categories. Write-off decisions should be evaluated here, but only after all appeal options are exhausted.
Concrete example: Say your A/R aging report shows $50,000 sitting in the 91–120 day bucket spread across three commercial payers. That is not a routine backlog—it is an immediate follow-up priority. Your billing team should pull each claim, identify the denial or delay reason, and either appeal, correct, or escalate within the next 5 business days.
Why Is My A/R Aging Increasing?
A rising total in your A/R aging report is rarely caused by one issue. It is almost always a combination of front-end and back-end breakdowns compounding over time.
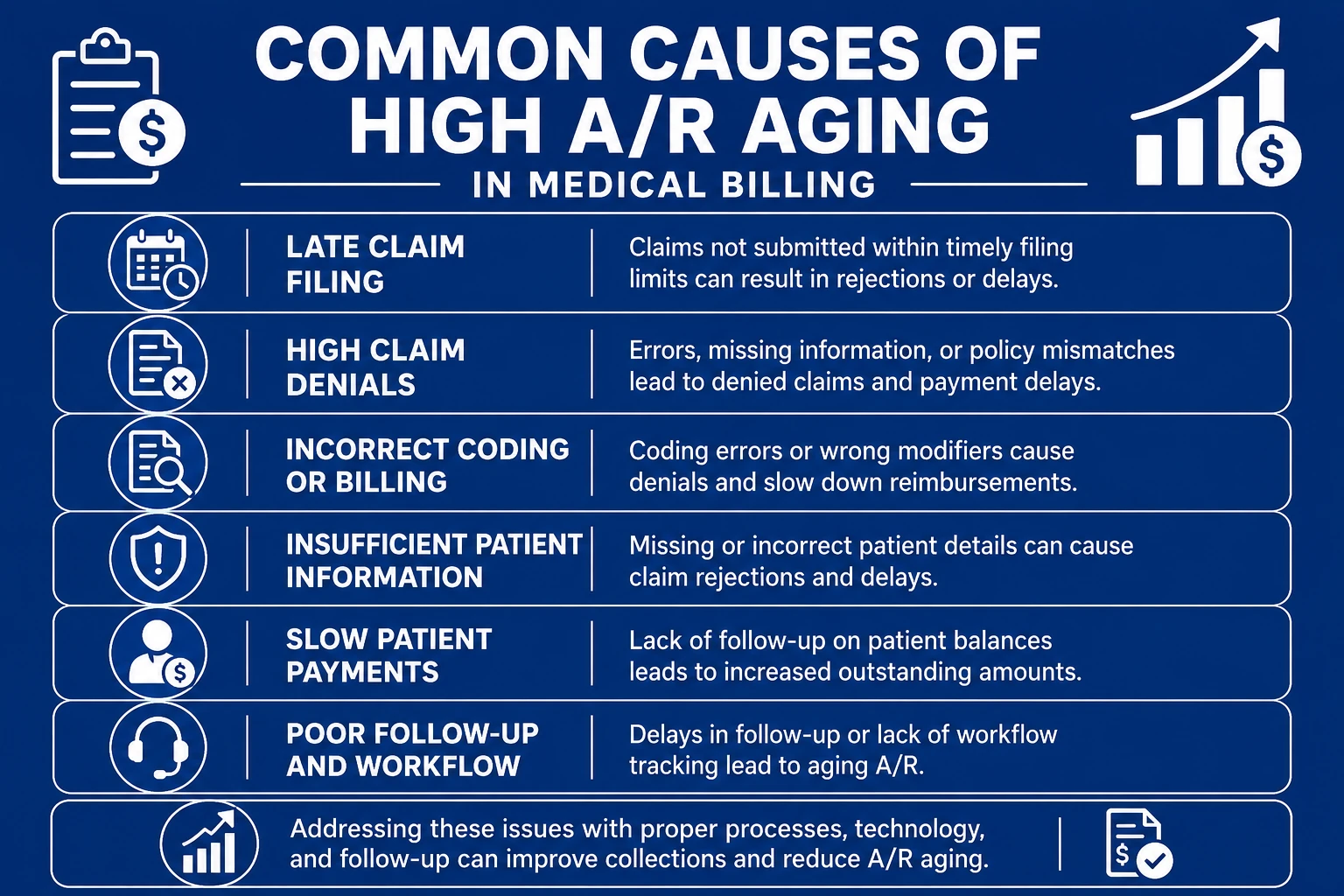
Common Causes of High A/R Aging in Medical Billing
- Late or incomplete claim submissions — Every day of charge lag adds a day to days in accounts receivable. A 10-day charge-to-submission window puts claims at day 10 before the payer even receives them.
- Unworked claim denials — Denied claims that sit without follow-up age into the 60–90 day bucket fast. This is one of the most direct drivers of high A/R aging. See our full guide on claim denials in medical billing to understand denial patterns by payer.
- Eligibility errors — Claims submitted without verified coverage are rejected on the front end and often resubmitted late, already 20–30 days into the aging window.
- Prior authorization gaps — Under the CMS Interoperability & Prior Authorization final rule (CMS-0057-F, effective January 1, 2026), federally regulated payers must respond to standard PA requests within 7 calendar days. But commercial payers still operate on their own timelines, and authorization delays directly stall claim submission and extend days in AR.
- Understaffed billing follow-up queues — When your billing team is stretched thin, the 91–120 day accounts go unworked while newer claims get attention.
- Incorrect coding — Mismatched diagnosis and procedure codes trigger denials, creating an aging cycle that compounds monthly.
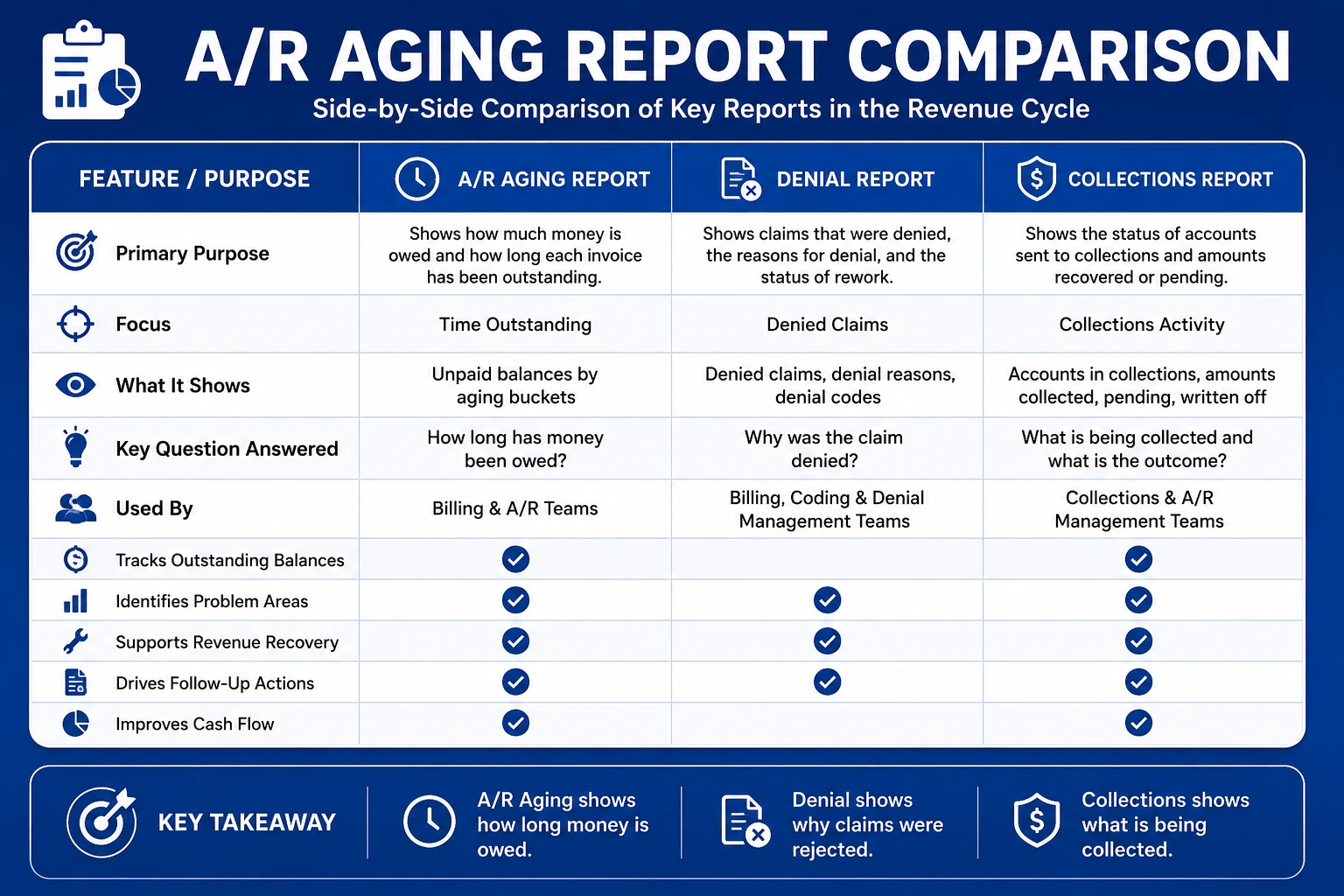
A/R Aging Report vs Other Reports on Your Billing Dashboard
Many practices confuse the A/R aging report with other reports in their practice management system. They serve different purposes and should never be used interchangeably.
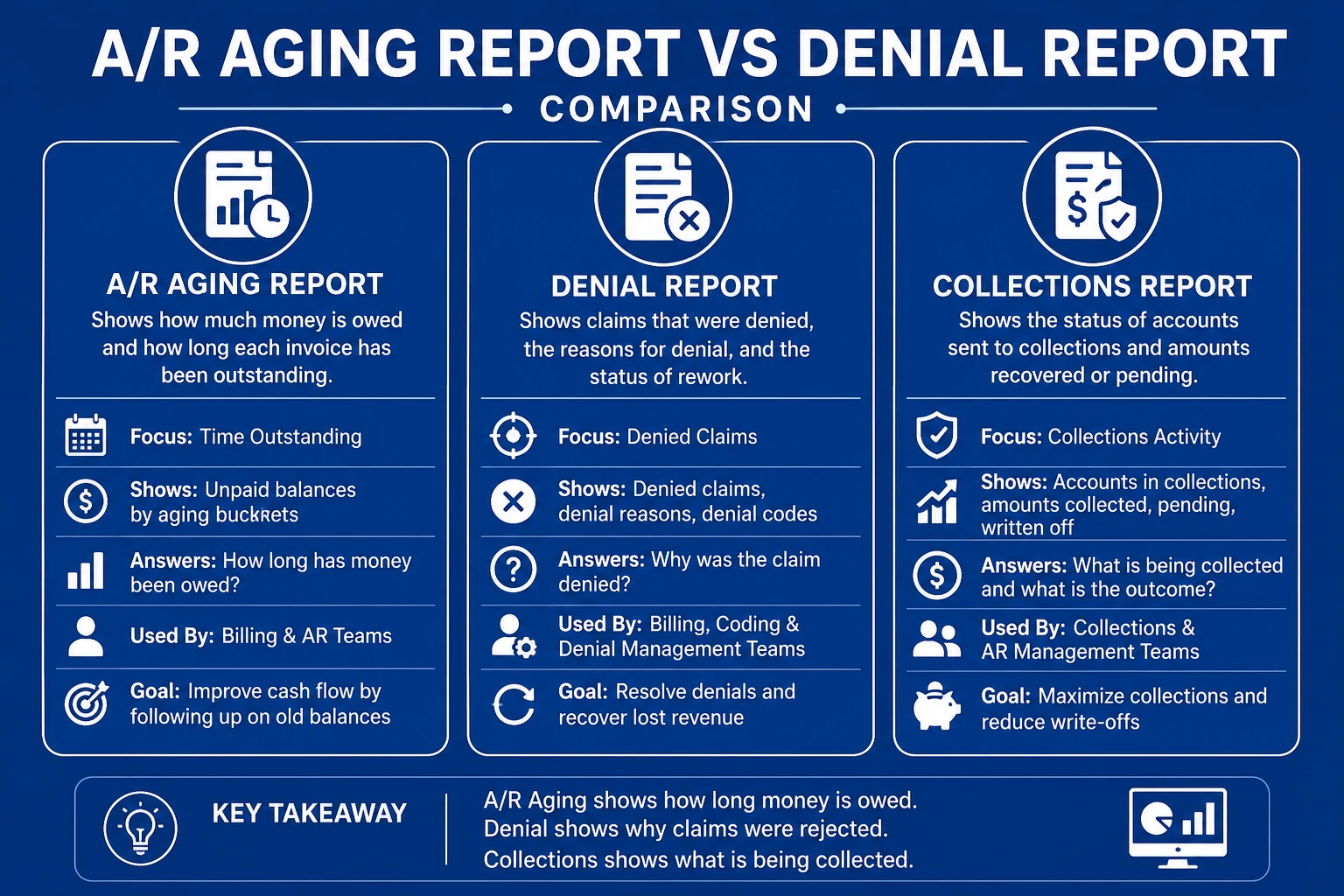
A/R Aging Report vs Denial Report
A denial report shows you which claims were rejected by a payer and why—based on CARC codes returned on the ERA/EOB. The A/R aging report shows you the total outstanding balance categorized by age, regardless of whether the claim was denied, underpaid, or simply slow to process.
You need both. A denial report is your root-cause tool. The A/R aging report is your prioritization tool. A claim can appear on both—it may be denied (on the denial report) and also sitting in the 61–90 day bucket (on the aging report) with no follow-up action taken.
A/R Aging Report vs Collections Report
A collections report measures how much your practice has collected versus billed—it is a performance snapshot. The A/R aging report shows what is still outstanding and how long it has been sitting unpaid. Use the collections report to evaluate your clean claim rate and payer reimbursement performance. Use the aging report to manage billing follow-up and daily operations.
What Is a Good Days in AR Benchmark?
Days in AR (days in accounts receivable) measures how many days on average it takes your practice to collect what it has billed. The formula is:
Days in AR = Total AR Balance ÷ Average Daily Charges
According to MGMA’s 2024 Cost and Revenue Survey, the median Days in AR for better-performing physician practices is 36 days, while the broader industry median sits at 47 days. HFMA sets the standard target at under 40 days. AAPC’s 2023 medical billing workplace survey found an industry mean closer to 42 days across all practice sizes.
Benchmark by specialty matters significantly:
- Primary care: 28–35 days
- Mental health: 30–40 days
- Surgical specialties (orthopedics, general surgery): 40–55 days
- DME / Home health: 50–70 days
A primary care practice running 50 days in AR has a structural billing problem. An orthopedic group at 50 days is operating near normal for its specialty. Context matters—but any practice above 50 days should investigate the root cause before it compounds.
Can You Write Off Balances Shown on the A/R Aging Report?
Yes—but only after you have exhausted every available recovery path. Writing off a balance prematurely is one of the most common sources of preventable revenue loss in medical billing.
Before writing off any balance from your A/R aging report, your billing team should confirm:
- The claim has been submitted correctly and the payer has received it.
- All applicable denials have been appealed at least once.
- The claim has not hit a timely filing deadline—which would make it permanently uncollectable.
- Patient responsibility balances have been billed and a payment plan has been offered if the patient has balance-due exposure.
Write-off rates should stay below 3–5% of total billed charges. When write-offs climb above that threshold, it is almost always a signal that unworked aged claims are being removed from the books instead of recovered. Your Revenue Cycle Management Services partner should audit every write-off above a defined dollar threshold before posting it.
How to Reduce AR Aging in Medical Billing — Step-by-Step
Reducing A/R aging is a process, not a one-time cleanup. Here is the step-by-step approach the TMS Billings team uses with high-volume and multi-specialty practices.
- Run your A/R aging report by payer. Aggregate aging hides payer-specific concentration problems. Break it down so you can see which payers are driving your 90+ day totals.
- Set a charge submission SLA of 48–72 hours. Every day of lag is a day added to days in AR. Tighten charge-to-submission times first—it is the fastest lever.
- Work denial management within 14 days of ERA receipt. Claims worked within two weeks of denial have materially better recovery rates than those left past 30 days.
- Build a bucket-by-bucket follow-up protocol. Assign specific staff or queues to each aging bucket. The 61–90 day and 91–120 day buckets should have dedicated follow-up cadences, not shared queues.
- Implement real-time eligibility verification. Run eligibility checks at scheduling and at check-in. Catch coverage mismatches before the claim is ever submitted.
- Audit write-offs monthly. Compare write-off volume against your total billed charges. Any spike above baseline signals unworked aged claims being removed rather than recovered.
- Review your A/R aging report by payer weekly. Payer-level aging analysis surfaces slow-adjudication patterns before they build into a 90+ day concentration problem.
Understanding your medical billing pricing models can also help you evaluate whether your current billing structure incentivizes aggressive follow-up or passive claim submission.
When and How to Escalate Old AR Balances
Not every aged claim can be resolved by resubmission. Escalation is a distinct step that requires judgment and a structured protocol.
Escalate when:
- The claim has passed 90 days with no payment or denial response from the payer.
- Two or more appeals have been submitted with no resolution.
- The balance is above your practice’s high-dollar threshold (typically $500–$1,000+).
- The claim is approaching a timely filing deadline or appeal window.
Escalation options:
- Payer provider relations call: Request a real-time status update and escalate unresolved high-dollar claims to a provider relations representative.
- Peer-to-peer review: For medical necessity denials, request a peer-to-peer review between your physician and the payer’s medical director.
- External collections: Patient-responsibility balances that reach 120+ days with no response may be appropriate for external collections—but only under a defined policy and after final billing notices.
- State insurance commissioner complaint: For payers with systemic non-payment or delay patterns, a complaint to the state insurance commissioner is a legitimate and often effective escalation path.
A/R Aging Report — Side-by-Side Comparison
| Feature | A/R Aging Report | Denial Report | Collections Report |
|---|---|---|---|
| Primary purpose | Prioritize follow-up by age of claim | Identify denial reason and root cause | Measure collections vs. billed charges |
| Organized by | Days outstanding (0–30, 31–60, 61–90, etc.) | CARC/RARC denial code | Payer, provider, date range |
| Best used for | Daily billing follow-up and escalation | Denial management workflow | KPI monitoring and revenue cycle benchmarking |
| Tracks denied claims? | Only if unresolved and still outstanding | Yes — primary function | Not directly |
| Tracks slow-pay patterns? | Yes — by bucket concentration | No | Partially (collection lag) |
| Action trigger | Follow-up, appeal, or write-off decision | Appeal, correct and resubmit | Performance improvement |
A/R Aging and Revenue Cycle Trends in 2026
The revenue cycle environment in 2026 is making AR aging harder to control. Here are the data points your billing team needs to understand.
Days in AR by specialty: MGMA’s 2024 Cost and Revenue Survey reports the median Days in AR at 36 days for better-performing practices and 47 days for the broader industry sample. More than half of all practices fall above the HFMA benchmark of 40 days, based on MGMA published data.
The 120+ day problem: Multispecialty practices report a median of 13.54% of total AR sitting in the 120+ day bucket. Claims that reach this threshold have collection rates below 50% across most payer categories. Write-off rates jump from 15–25% at the 90-day mark to 40–60% beyond 120 days.
Revenue impact: For a 10-provider specialty group carrying $2.4M in total AR, industry analysis identifies a median of $112,000 in hidden aging gaps—split across timely filing cliff claims, payer-concentration backlog, silent write-offs, and gross-to-net mismatches.
Payer trends widening the AR window: The AMA’s 2025 Prior Authorization Physician Survey found 95% of physicians report that prior authorization delays access to care—and those delays translate directly into slower payer reimbursement and extended days in AR. As of January 1, 2026, CMS (under rule CMS-0057-F) requires federally regulated payers to respond to standard PA requests within 7 calendar days, but commercial plans are not subject to the same mandate. Experian Health’s State of Claims 2025 found 41% of providers now report denial rates of 10% or higher—up from 30% in 2022—adding further pressure to AR aging management across every specialty.
Staff workload: Industry benchmarks recommend one AR specialist per $1–2 million in annual collections. Practices below that ratio are almost always seeing elevated 90+ day AR as a direct consequence of understaffed billing follow-up queues.
Best Practices to Keep Your A/R Aging Report Clean
Keeping your A/R aging report healthy is an ongoing discipline, not a quarterly cleanup project. The practices that consistently hit MGMA top-quartile benchmarks (28–32 days in AR) share these habits.
- Review the aging report weekly, not monthly. Monthly review lets the 31–60 day bucket age into 61–90 before anyone acts.
- Segment by payer, provider, and facility. Aggregate totals hide the concentration problems that drive aged AR spikes.
- Set a hard threshold for 90+ day AR. Healthy practices keep the 90+ day bucket under 15% of total outstanding claims. Above 20% is a red flag.
- Track your clean claim rate alongside the aging report. A low clean claim rate (below 95%) directly feeds claim rejections and subsequent AR aging. Improving denial management is the most direct path to better clean claim rate and lower days in AR.
- Document your follow-up actions at the claim level. Every contact, appeal, or resubmission should be logged so the next billing specialist who touches the claim understands its full history.
- Tie write-off decisions to your aging report review cycle. No balance should be written off that hasn’t been reviewed against timely filing deadlines, appeal status, and dollar thresholds.
How TMS Billings Helps Practices Manage Their A/R Aging Report
At TMS Billings, the revenue cycle and denial management team treats the A/R aging report as an active operations document—not a passive financial statement. Here is what that means in practice for your billing team.
Payer-level aging analysis: We run your A/R aging report by payer, not just by bucket total. That distinction reveals which payers are driving your 90+ day concentration and allows targeted follow-up—not blanket resubmission.
Timely filing monitoring: We track timely filing deadlines at the claim level. Medicare allows 365 days from the date of service for original submissions; commercial payers vary from 90 days to 12 months. We flag any claim approaching its deadline before the window closes.
Structured follow-up protocols: Your accounts receive dedicated follow-up by age bucket. The 61–90 day and 91–120 day claims are worked on a defined cadence—not when staff has capacity.
Denial root-cause analysis: When a claim appears in both your denial report and your aging report, we identify the specific CARC code, determine whether a corrected claim or a formal appeal is required, and take action within 14 days of ERA receipt.
Write-off auditing: No balance is written off without a documented review. We confirm timely filing status, appeal history, and dollar threshold compliance before any adjustment is posted.
Transparent reporting: You receive regular aging summaries broken out by payer, bucket, and provider—so you always know where your revenue stands and what is being done about it.

Key Takeaways
- The A/R aging report categorizes outstanding claims into time buckets (0–30, 31–60, 61–90, 91–120, 120+ days) to prioritize billing follow-up.
- Claims past 90 days have collection rates below 50%; the 120+ day bucket is approaching write-off territory.
- MGMA benchmarks Days in AR at 36 days for better-performing practices; anything above 50 days signals a structural billing problem.
- High A/R aging is almost always caused by a combination of slow charge submission, unworked denials, and understaffed follow-up queues.
- The A/R aging report, denial report, and collections report serve different purposes—all three are needed for a complete picture of revenue cycle health.
- Write-offs should only be posted after appeal history, timely filing status, and high-dollar thresholds have been reviewed.
Final Thoughts
Your A/R aging report is the most accurate real-time signal your practice has for where revenue is stuck and how urgently you need to act. If your 90+ day buckets are growing, your billing team is losing the race against payer timelines, appeal deadlines, and timely filing windows.
The TMS Billings revenue cycle team specializes in exactly this work—working aged claims, appealing denials, auditing write-offs, and keeping days in AR at or below MGMA benchmarks for your specialty. If your aging report shows concentration in the 61+ day buckets, that is the right time to act—not after another billing cycle passes.
Ready to bring your A/R aging report under control? Contact TMS Billings today for a complimentary aging analysis and revenue cycle review.


