2026 Mental Health CPT Codes: The Full Guide to Billing Without Denials
Mental health billing is one of the highest-risk revenue areas in outpatient practice today. Payers are tightening prior authorization requirements, CMS continues updating the fee schedule, and documentation standards keep rising. If your billing team is still running 2023 or 2024 workflows, your practice is almost certainly leaving money behind — or absorbing the cost of preventable denials.
This guide breaks down everything you need about mental health CPT codes in 2026: what changed, which codes apply to which services, how Medicare and commercial payers differ, and exactly what documentation your team needs to survive a payer audit. Whether you run a solo psychiatry practice or a multi-provider behavioral health group, this is the resource your billing staff needs before submitting another claim.
Start with the right foundation: your Revenue Cycle Management Services strategy determines whether your clean claim rate grows — or stalls.
What Are Mental Health CPT Codes in 2026?
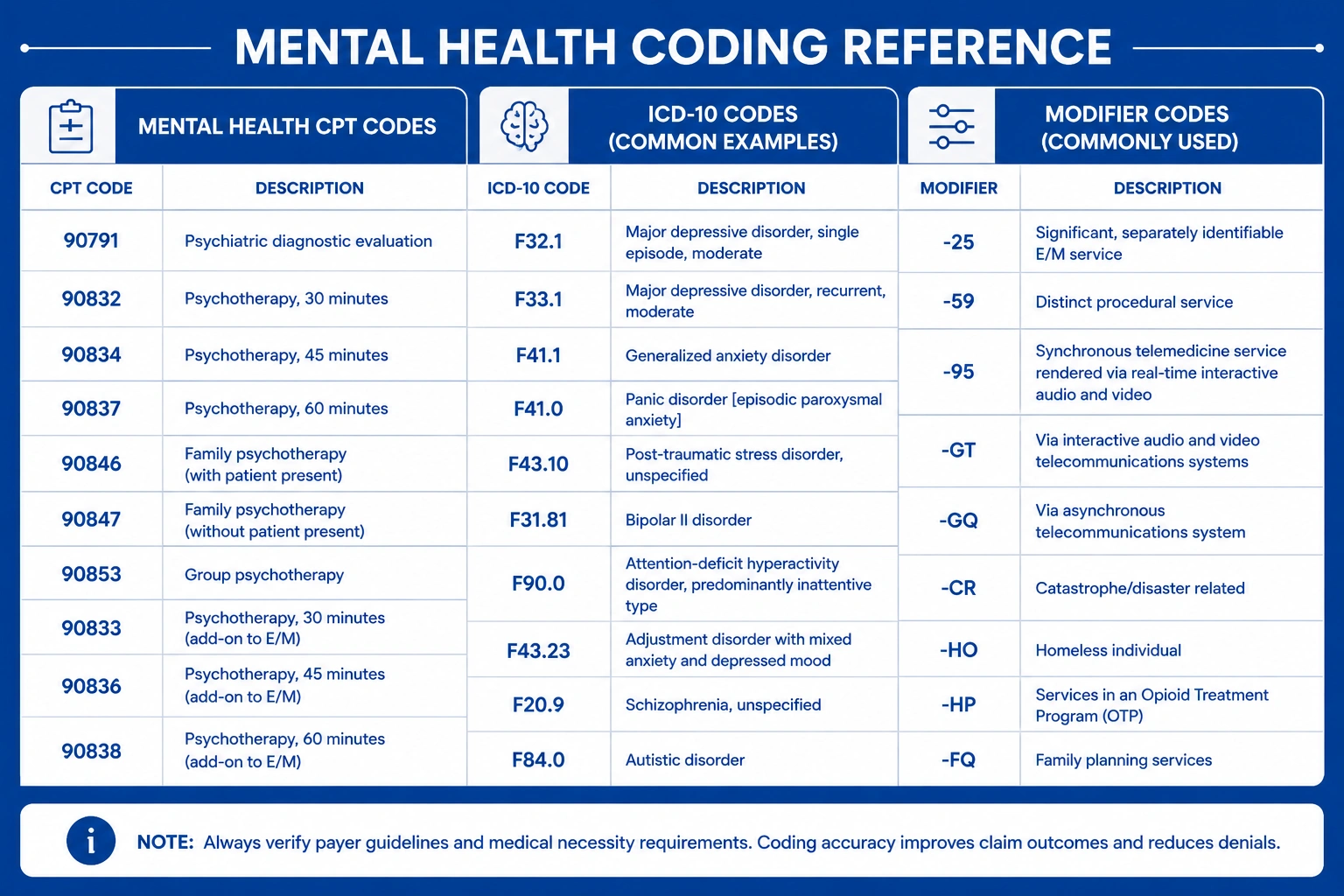
📋 What Are Mental Health CPT Codes?
Mental health CPT codes are standardized five-digit procedure codes used to bill insurance for psychiatric and psychotherapy services. They identify the type, duration, and setting of care delivered — from individual therapy to crisis intervention. Accurate use of mental health CPT codes is essential for clean claim submission and timely reimbursement from Medicare, Medicaid, and commercial payers.
Mental health CPT codes define every billable service your clinicians deliver — from a 30-minute therapy session to a full psychiatric crisis stabilization encounter. The American Medical Association publishes and maintains these codes, and CMS uses them to set reimbursement rates under Medicare and Medicaid.
In 2026, accuracy with these codes is non-negotiable. Payers use automated claim-scrubbing software that flags mismatches between diagnosis codes, procedure codes, and provider types before a human reviewer ever sees your claim.
Why Mental Health CPT Code Accuracy Is a Revenue Priority for Every Practice
Behavioral health billing codes 2026 have evolved significantly. Payers are more aggressive with prior authorization, Medicare has clarified which services qualify under the outpatient mental health benefit, and mental health procedure codes now carry modifier requirements that vary by service delivery method. For your practice, every coding error is a potential denial — and every denial costs time, money, and administrative bandwidth your team doesn’t have to spare.
Getting mental health procedure codes right the first time protects your revenue cycle and reduces compliance exposure if your practice is ever audited.
What Changed in Mental Health Billing After Recent CMS and Payer Policy Shifts
CMS made important adjustments to mental health reimbursement following COVID-era telehealth expansions. Some flexibilities have been codified permanently — but not all of them, and not uniformly across payers. Commercial payers have also introduced new step therapy requirements for certain psychiatric medications, and prior authorization for behavioral health services has expanded to cover services that were previously auto-approved.
CMS Mental Health Billing Updates and What’s Permanent in 2026
CMS mental health billing 2026 updates include expanded telehealth psychotherapy coverage, clarified E&M documentation requirements for psychiatric evaluations, and updated payment rates under the Medicare Physician Fee Schedule. Notably, audio-only telehealth for mental health services remains covered under Medicare in 2026 for patients in qualifying locations — but modifier requirements apply. Miss a single modifier and the claim won’t pay.
Why Many Practices Are Still Leaving Mental Health Reimbursement on the Table
Most revenue losses in mental health billing don’t come from fraud — they come from systems that haven’t kept pace with payer rule changes. Counseling CPT codes 2026 carry different modifier requirements depending on whether a session is in-person, via video, or audio-only. Billing teams that don’t account for those distinctions generate rejections they can’t immediately explain or correct.
The Hidden Revenue Risk of Incorrect Mental Health Procedure Codes
Using the wrong mental health procedure codes — even by one digit — triggers an automatic denial or, worse, a payer audit. If auditors identify systemic up-coding across your claims, your practice could face recoupment demands going back months or years.
The Biggest Causes of Mental Health Billing Denials in 2026
Understanding where denials originate is the first step to preventing them. Here are the most common failure points in mental health billing workflows.
Missing or Incomplete Prior Authorization for Mental Health Services
Commercial payer mental health prior authorization requirements have expanded substantially. Many payers now require authorization not just for inpatient psychiatric admissions but for outpatient psychotherapy after a defined number of sessions. Mental health prior authorization requirements by payer in 2026 vary widely — what UnitedHealthcare requires may differ completely from Aetna or BCBS. Your billing team needs payer-specific workflows, not a one-size-fits-all authorization process.
Wrong ICD-10 Diagnosis Codes — Depression vs. Anxiety vs. Psychiatric Disorders
ICD-10 codes for mental health disorders must match the clinical picture and the CPT code billed. Billing a psychotherapy code with a diagnosis of Z00.00 (routine exam) triggers an immediate denial. Diagnosis codes for depression and anxiety billing require specificity — F32.1 (major depressive disorder, single episode, moderate) will pass through payer scrubbers that F32.9 (unspecified) will not.
Medicare Outpatient Mental Health Billing Confusion
Medicare outpatient mental health billing has its own distinct rules. The 20% coinsurance applies, the annual deductible must be met, and providers must be correctly enrolled in Medicare Part B for mental health services. Billing under a general practice taxonomy when psychiatry-specific enrollment is required creates denials that take weeks to untangle.
Documentation Gaps That Trigger Automatic Denials
Payer scrubbers are sophisticated. If your clinical notes don’t include a current diagnosis, session duration, and a clear treatment goal, you are at risk. Documentation requirements are especially strict under CMS, where the absence of a single required element can void an otherwise valid claim.
Confusing Psychotherapy CPT Codes With E&M Codes for Psychiatric Billing
E&M codes for psychiatric services (99202–99215) are appropriate when the session primarily involves medical decision-making — such as prescribing or adjusting psychiatric medication. Psychotherapy CPT codes apply to documented therapy time. Using them interchangeably, or failing to use add-on codes correctly, is one of the most common and most costly billing mistakes in behavioral health.
Step Therapy and Formulary Restriction Violations by Payer
Some payers require patients to fail on a first-line medication before authorizing a second-line psychiatric medication. If your documentation doesn’t reflect that step therapy pathway, your authorization — and your claim — can be denied retroactively.
The Complete Mental Health CPT Codes 2026 Billing Guide
Psychotherapy CPT codes 2026 cover a wide range of service types across individual, group, crisis, and telehealth settings. Below is a structured overview of the core codes your billing team needs to know — and the rules that govern each.
Individual Psychotherapy CPT Codes — 90832, 90834, and 90837
Individual therapy CPT codes 90832, 90834, and 90837 are the backbone of outpatient behavioral health billing. Each code is tied directly to documented session time.
| CPT Code | Session Duration | Service Type |
|---|---|---|
| 90832 | 16–37 minutes | Brief individual psychotherapy |
| 90834 | 38–52 minutes | Standard individual psychotherapy |
| 90837 | 53+ minutes | Extended individual psychotherapy |
| 90853 | Variable | Group psychotherapy |
| 90839 | First 60 minutes | Crisis psychotherapy |
| 90840 | Each additional 30 min | Crisis add-on code |
What CPT codes are used for individual psychotherapy sessions depends entirely on the time documented in the clinical record — not the scheduled session length. Billing 90837 for a 40-minute session is up-coding, and it creates immediate audit exposure.
Group therapy vs. individual therapy CPT codes are not interchangeable. CPT 90853 is specifically for group psychotherapy and carries a lower reimbursement rate. Always verify and bill the correct service setting.
ICD-10 Codes That Support Medical Necessity for Mental Health Services
ICD-10 codes for mental health disorders must reflect exactly what is documented in the clinical note. The most commonly used codes include:
- F32.1 — Major depressive disorder, single episode, moderate
- F41.1 — Generalized anxiety disorder
- F43.10 — Post-traumatic stress disorder, unspecified
- F20.9 — Schizophrenia, unspecified
- F31.9 — Bipolar disorder, unspecified
- F90.0 — ADHD, predominantly inattentive presentation
Diagnosis codes for depression and anxiety billing must be specific. Avoid “unspecified” codes when the clinical documentation clearly supports a more precise diagnosis. Payer scrubbers in 2026 are increasingly flagging non-specific codes as insufficient for medical necessity.
E&M and Add-On Codes for Psychiatric Billing
When a psychiatrist conducts both psychotherapy and medical management in a single visit, you may bill a psychotherapy add-on code alongside an E&M code. Mental health modifier codes and add-on codes such as 90833 (psychotherapy add-on, 16–37 minutes) allow appropriate reimbursement when both services are provided and documented within the same encounter. Psychiatric billing codes 2026 also include 90785, an interactive complexity add-on used when legal, regulatory, or third-party factors complicate the clinical work.
Telehealth Mental Health CPT Codes and Modifier Requirements
Telehealth mental health billing codes use the same base CPT codes as in-person services but require specific modifiers to identify the delivery method:
- Modifier 95 — Synchronous video telehealth
- Modifier 93 — Audio-only telehealth (where covered by payer)
- GT — Often required by Medicare Advantage and select commercial plans
- POS 02 — Telehealth, non-home setting
- POS 10 — Telehealth, patient’s home
How to bill insurance for mental health services in 2026 via telehealth requires verifying each payer’s specific modifier preferences before claim submission. A video modifier submitted to a payer that requires a different code will reject immediately — even when the service itself is covered.
How Much Revenue Is Your Practice Losing to Mental Health Billing Errors?

Our Medical Billing Services team regularly identifies five- and six-figure annual revenue losses in practices that believe their billing is clean. Here is what those losses look like in real-world scenarios.
Example 1 — Wrong Diagnosis Code Leads to a Blanket Prior Auth Denial
A group practice bills CPT 90837 for extended psychotherapy sessions using F41.9 (anxiety disorder, unspecified) as the primary diagnosis. The payer’s medical policy requires a more specific anxiety diagnosis code for sessions exceeding 52 minutes. The result: a blanket prior authorization denial affecting 30 patients. Reworking those claims — gathering documentation, resubmitting corrected codes, and following up — consumed 11 hours of administrative time.
Example 2 — Mental Health Claims Denied for Incomplete Step Therapy Documentation
A psychiatry practice prescribes a second-generation antipsychotic as a first-line treatment without documenting why first-line alternatives were not appropriate. The commercial payer’s prior authorization policy requires evidence of step therapy compliance. Authorization is denied, reimbursement is delayed 45–60 days, and the practice must build a retroactive clinical appeal from scratch.
Example 3 — Specialty-Specific Reimbursement Gaps in Psychiatric Billing
A practice billing psychiatric billing codes 2026 under a general “behavioral health” provider taxonomy discovers that reimbursement rates are 18–22% below what a psychiatry-specific taxonomy would yield. This is a billing configuration error — not a code error — but it quietly erodes revenue every single month until it is identified and corrected.
Medicare vs. Commercial Payer Mental Health Rules: A 2026 Comparison
What Medicare Covers for Mental Health Services in 2026
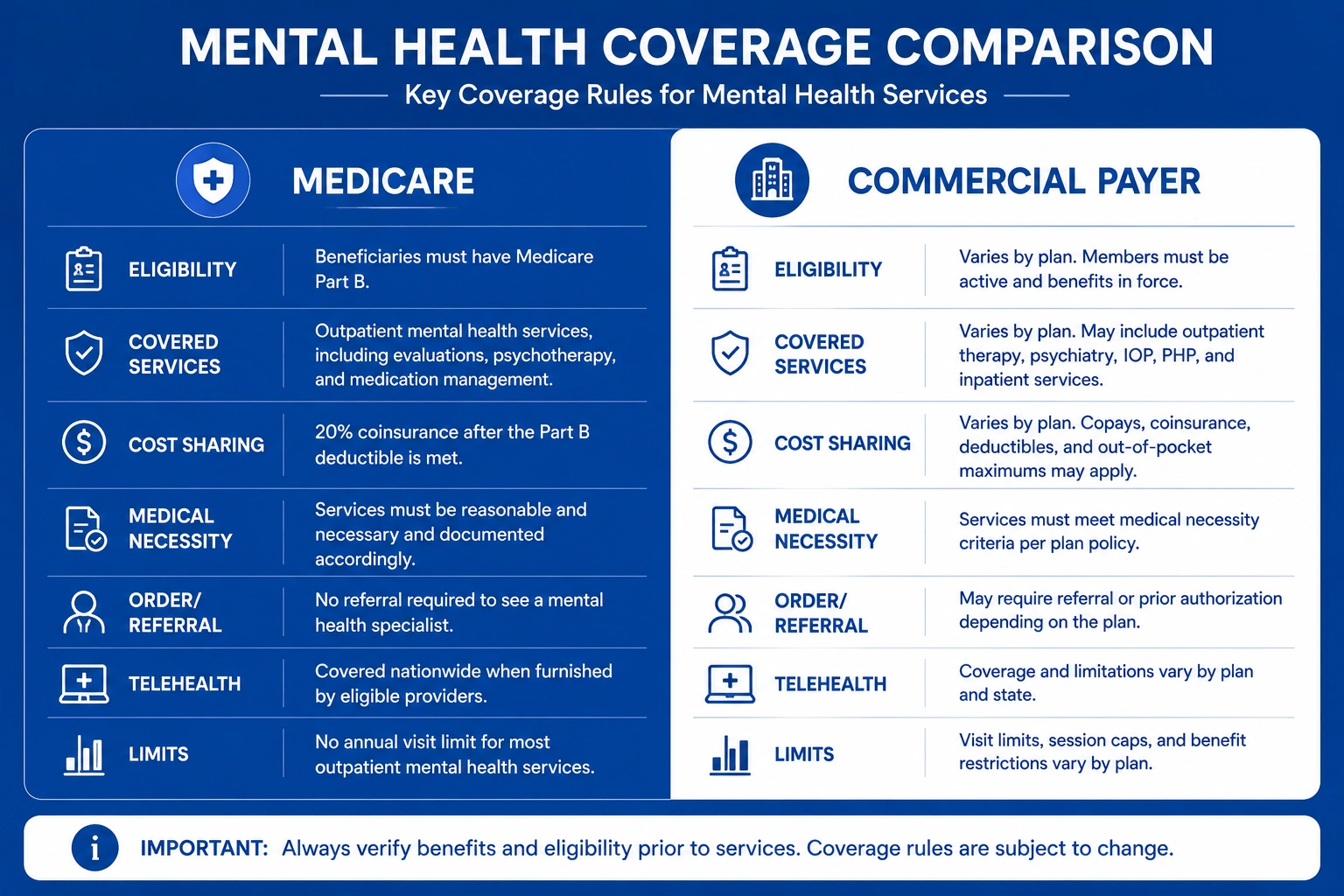
How does Medicare cover outpatient mental health services in 2026? Medicare Part B covers outpatient psychotherapy, psychiatric evaluation, and crisis services. Beneficiaries pay 20% coinsurance after meeting their annual deductible. According to CMS, the 2026 Physician Fee Schedule maintains coverage for telehealth mental health services, including audio-only visits for qualifying beneficiaries in eligible locations.
How Commercial Payers Differ From Medicare on Mental Health Coverage
| Coverage Feature | Medicare | Commercial Payers |
|---|---|---|
| Prior auth — outpatient therapy | Generally not required | Often required after session threshold |
| Telehealth coverage | Permanent (2026) | Varies significantly by plan |
| Audio-only visits | Covered (qualifying sites) | Rarely covered |
| Step therapy requirements | Limited | Common for psychiatric medications |
| Annual session limits | No hard cap | Often 20–40 sessions per year |
| Reimbursement rate basis | Medicare Physician Fee Schedule | Negotiated contract rates |
Commercial payer mental health prior authorization requirements are among the most inconsistent and burdensome aspects of behavioral health billing codes 2026. Your billing team needs per-payer workflows — not general authorization processes — to navigate them without constant denials.
Medicaid Mental Health Coverage Variation by State
Counseling CPT codes 2026 reimbursement rates under Medicaid are not uniform. Coverage is set at the state level, and some states enforce mental health parity aggressively while others have significant coverage gaps. Verify your state Medicaid rates and coverage policies annually — they change without advance notice.
Documentation Requirements for Mental Health Claims
What Must Be in the Clinical Note to Support Mental Health Medical Necessity
Every clinical note supporting a mental health CPT code claim must include:
- Current DSM-5 diagnosis with the corresponding ICD-10 code
- Session date, documented start time, and documented stop time
- Session type (individual, group, telehealth)
- Presenting symptoms and measurable treatment progress or response
- Provider signature with full credentials
Missing any of these elements creates a claim that can be denied on documentation grounds alone — even when the service itself was medically appropriate and correctly coded.
Prior Authorization Packets — What Payers Require in 2026
Mental health prior authorization requirements by payer in 2026 typically include clinical progress notes, a complete treatment plan, a current diagnosis, and — for psychiatric medications — documented evidence of step therapy compliance. Complete, well-organized prior auth packets move faster through payer review. Incomplete packets stall or get denied outright.
Our Medical Coding Services team builds payer-specific authorization packets that anticipate what reviewers need before they request it, significantly reducing approval turnaround time.
Avoiding Common Documentation Errors That Trigger Audits and Clawbacks
The most common documentation errors include vague or generic treatment goals, missing session timestamps, and absent clinical rationale for extended-duration sessions. Each of these can flag a claim for audit — and audits that uncover systemic errors result in recoupment demands that extend across multiple billing periods.
Strategies Every Practice Should Implement Right Now
Verify Mental Health Coverage and Prior Auth Requirements Before Scheduling
Check prior authorization requirements at scheduling — not at billing. A session delivered without active authorization is an uncompensated session in most commercial plans. Building eligibility and authorization verification into the scheduling workflow eliminates this risk before it happens.
Use the Correct Diagnosis Code Combination for Each Payer
Some payers accept ICD-10 codes for mental health disorders only when paired with specific secondary diagnosis codes. Build a payer-specific ICD-10 pairing reference for your five highest-volume payers and update it quarterly.
Build a Standardized Prior Authorization Workflow for Mental Health Services
Create a documented, repeatable workflow — not a tribal knowledge system — for prior authorization. Assign clear ownership, define response timelines, and build in tracking so no authorization lapses without your team knowing immediately.
Train Your Billing Staff on Payer-Specific Mental Health Procedure Codes and Step Therapy Rules
Mental health procedure codes and step therapy requirements change frequently. Build quarterly training into your billing operations calendar. What was accurate in 2024 may create denials in 2026 — and your reimbursement rate reflects that gap.
Outsource Mental Health and Behavioral Health Billing to Specialists
Can small practices get reimbursed for mental health counseling at competitive rates? Yes — but only when billing is executed correctly and consistently. Many small practices lack the staff bandwidth to stay current on every behavioral health billing codes 2026 update across multiple payers. Outsourcing to a specialty RCM team solves that problem without requiring additional in-house hires.
How Outsourced Mental Health Billing Protects Your Revenue
Proactive Prior Auth Denial Prevention for Mental Health Claims
A specialized billing team monitors authorization thresholds by payer and flags sessions approaching expiration before claims are submitted without coverage. This prevents the most common and most expensive type of mental health billing denial: the missed authorization cutoff.
Faster, Fully Documented Appeals With Clinical Evidence
When denials do occur, an experienced team prepares appeals with clinical documentation, payer policy citations, and medical necessity arguments that general administrative staff simply aren’t equipped to write or research under deadline pressure.
Payer-Specific Mental Health Denial Tracking and Trend Reporting
Outsourced billing teams maintain denial tracking databases that identify payer-specific denial patterns before they become systemic. If a payer begins denying a specific mental health CPT code combination, your team identifies the trend immediately — not after months of compounding revenue loss.
How TMS Billings Helps Practices Maximize Mental Health Reimbursement

TMS Billings specializes in behavioral health and psychiatric billing for solo providers and multi-site practices alike. Our team stays current on every CMS mental health billing 2026 update, commercial payer policy change, and state Medicaid rate adjustment — so your billing staff doesn’t have to.
We don’t use generic billing workflows. We build payer-specific billing protocols for every mental health CPT code combination your clinicians use and track denial trends so your practice is never blindsided by a payer policy shift. Whether you’re managing a handful of weekly sessions or hundreds, our RCM team protects your revenue and reduces your administrative burden at scale.
Contact TMS Billings today to find out exactly where your current billing workflow is costing you money — and how we’ll fix it.
The Financial Cost of Mental Health Billing Errors in 2026
The financial stakes of mental health billing errors are significant and growing. Here is what the data shows.
- Utilization growth is amplifying billing risk. Mental health service utilization has increased year-over-year since 2020. Higher claim volume means coding errors compound across thousands of claims — and the dollar impact scales proportionally.
- Incorrect diagnosis codes and missing prior auth are expensive. According to MGMA, behavioral health practices lose a significant portion of net revenue each year to preventable claim denials, most commonly driven by ICD-10 specificity failures and authorization gaps that could have been caught before submission.
- Reworking denied claims carries a real administrative cost. Industry benchmarks place the average cost of reworking a single denied mental health or behavioral health claim at $25–$35 in staff time. Across hundreds of monthly denials, that cost accumulates into a meaningful operational drag on your practice.
- Medicare and commercial reimbursement gaps are widening. Medicare outpatient mental health billing rates and commercial reimbursement rates increasingly diverge in 2026, making payer mix analysis and contract negotiation essential financial levers for every behavioral health practice.
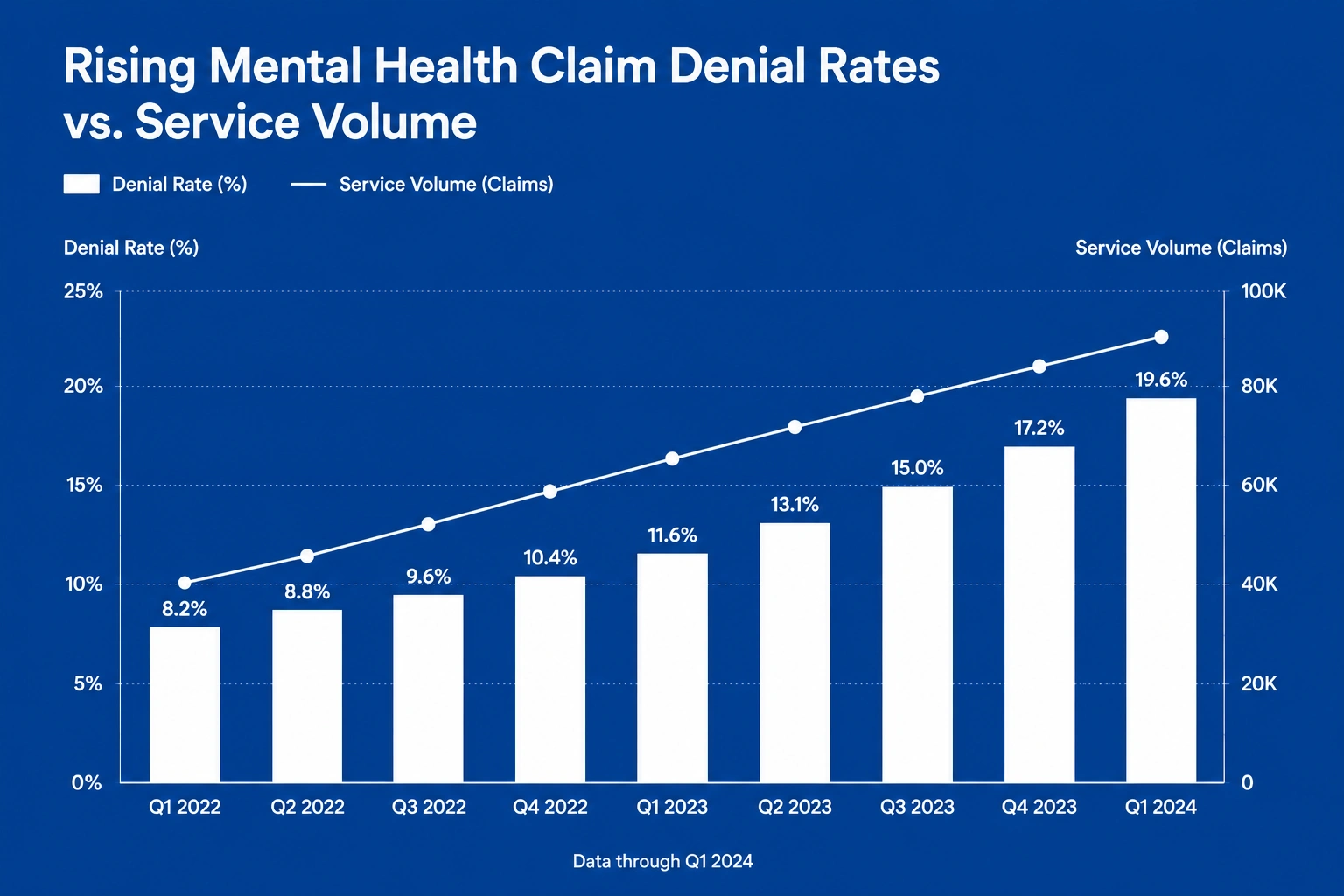
- Reimbursement success doesn’t keep pace with service volume. Research from the AMA confirms that prior authorization burden in behavioral health creates a persistent gap between the volume of mental health services delivered and the volume successfully reimbursed. Practices without optimized billing workflows absorb that gap as lost revenue every single month.
Key Takeaways
- Mental health CPT codes in 2026 require payer-specific prior authorization workflows and precise modifier use — not generic billing processes
- Individual therapy CPT codes 90832, 90834, and 90837 are time-based; always document exact session start and stop times
- ICD-10 codes for mental health disorders must be specific — “unspecified” codes are increasingly rejected by payer scrubbers
- Medicare and commercial payers have meaningfully different rules for telehealth coverage, prior authorization, and session limits
- Documentation gaps are the leading driver of payer audits and clawbacks in behavioral health billing
- Both small and large practices can protect mental health reimbursement with the right billing support and payer-specific workflows
Final Thoughts
Mental health billing is not a background administrative function — it is a direct determinant of your practice’s financial health. Every incorrect mental health CPT code, every missed prior authorization, and every vague clinical note is a revenue loss that compounds quietly over time.
Your patients deserve access to care. Your practice deserves to be fully reimbursed for delivering it. Getting your mental health CPT codes and billing workflows right in 2026 is how you protect both.
Ready to stop losing revenue to preventable billing errors? Contact TMS Billings today. Our team will show you exactly where your current workflow is falling short — and build a strategy to fix it.