HBOT for Traumatic Brain Injury (TBI): What the Latest Research Actually Says
Every year, millions of people sustain traumatic brain injuries that permanently alter the course of their lives — and far too many never fully recover through standard care alone. If you or someone you love is living with the persistent effects of a TBI, you’ve likely asked whether more can be done. HBOT for traumatic brain injury has emerged as one of the most closely studied and clinically discussed rehabilitation tools in modern neuroscience. Our Hyperbaric Oxygen Therapy Services team works alongside TBI patients, neurologists, and rehabilitation specialists to help patients understand the evolving evidence and explore whether HBOT belongs in their recovery plan.
This article walks through what the science actually shows — not the hype, not the blanket dismissals — so you can approach this decision with clarity and confidence.
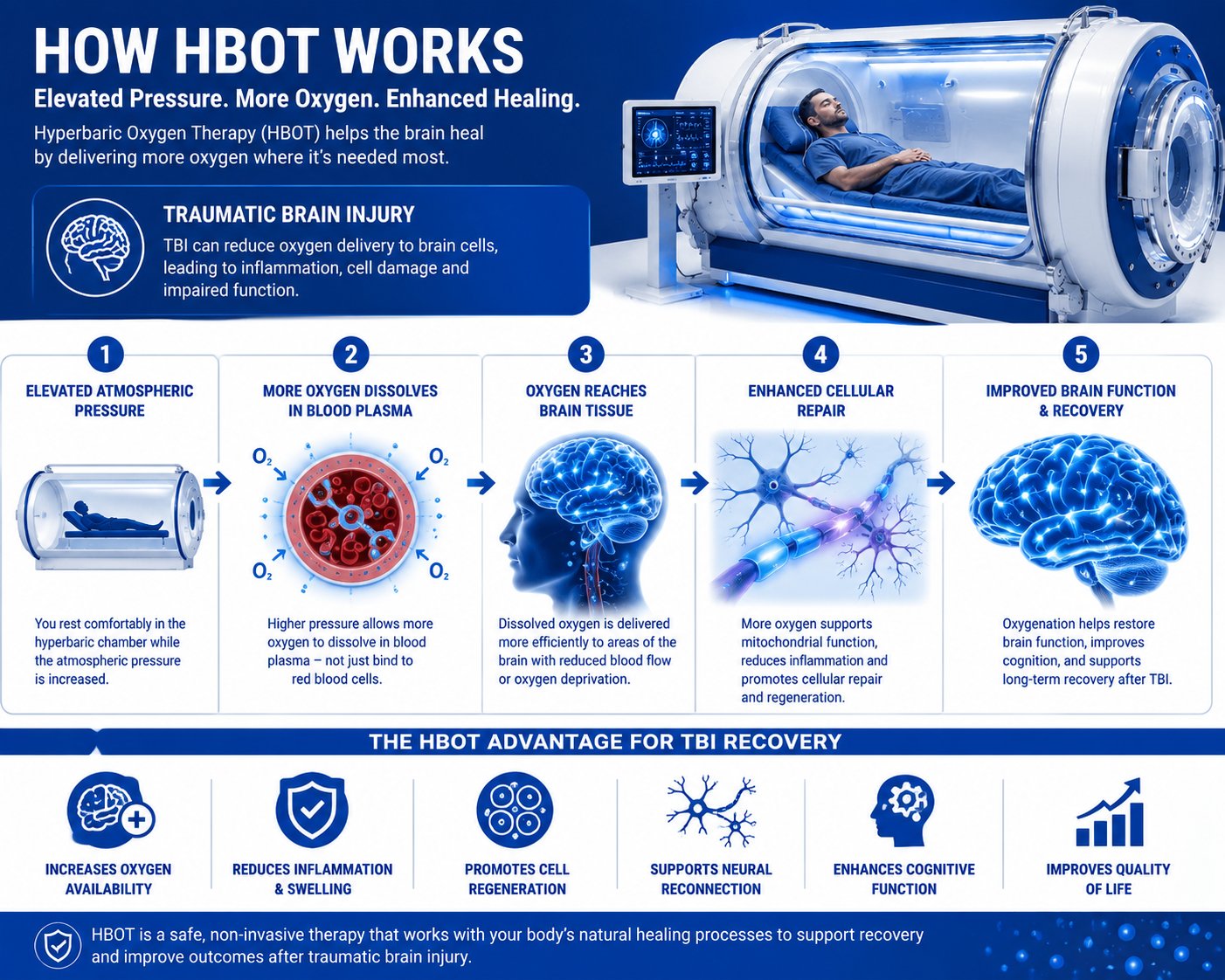
What Is HBOT for Traumatic Brain Injury? HBOT (hyperbaric oxygen therapy) for traumatic brain injury involves breathing 100% pure oxygen inside a pressurized chamber at 1.5 to 2.4 atmospheres absolute (ATA). The elevated pressure drives oxygen into blood plasma and damaged brain tissue, reducing neuroinflammation, improving cerebral blood flow, and stimulating neuroplasticity to support recovery from injury.

What Is HBOT for Traumatic Brain Injury?
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes pure oxygen inside a sealed, pressurized chamber. Atmospheric pressure inside the chamber is raised to between 1.5 and 2.4 times normal pressure — a range measured in atmospheres absolute, or ATA.
At this elevated pressure, oxygen dissolves directly into blood plasma, cerebrospinal fluid, and tissue fluid, rather than relying solely on hemoglobin to carry it. This is a critical distinction. For a brain that has sustained trauma, this expanded oxygen delivery can be meaningful. The injured brain is frequently oxygen-deprived, chronically inflamed, and metabolically impaired. HBOT supplies exactly what it needs to begin repairing itself at the cellular level.
HBOT brain injury treatment is not a new concept. Hyperbaric medicine has a decades-long clinical history, most established in wound healing, decompression sickness, and carbon monoxide poisoning. What is newer — and what this article addresses directly — is the growing body of peer-reviewed research examining HBOT for neurological injury, specifically traumatic brain injury.
Why TBI Patients Are Turning to Hyperbaric Oxygen Therapy
The Gap Between Standard TBI Care and Full Recovery
Standard TBI rehabilitation typically includes cognitive therapy, physical therapy, occupational therapy, medication management, and rest protocols. For mild TBIs, many patients recover within weeks to months. But for a significant subset — particularly those with moderate, severe, or chronic TBI — standard care leaves a persistent recovery gap.
Symptoms like chronic headaches, memory deficits, emotional dysregulation, cognitive fatigue, and difficulty concentrating often remain long after conventional treatment concludes. This gap is deeply frustrating for patients, families, and clinicians. It is also what is driving serious scientific interest in hyperbaric oxygen therapy TBI research.
Why Many Patients Seek Alternative Neurological Treatments
When standard rehabilitation plateaus, patients and families begin searching for evidence-based alternatives. Many arrive at HBOT after reading about clinical trials, hearing from veterans with blast injuries who have experienced benefit, or consulting neurologists who are familiar with the emerging hyperbaric medicine literature.
The appeal of hyperbaric oxygen therapy for brain injury is not rooted in hope alone. It is grounded in biology. The injured brain has measurable, documented deficits — in oxygenation, in blood flow, in cellular energy production — that HBOT is designed specifically to address.
The Biological Case for HBOT in Brain Injury
The brain is one of the most metabolically demanding organs in the human body. It consumes approximately 20% of the body’s oxygen while representing only 2% of its mass. After traumatic brain injury, the neurons and glial cells that make up brain tissue are oxygen-starved, inflamed, and metabolically disrupted.
HBOT neurological benefits are rooted in its ability to saturate brain tissue with oxygen far beyond what normal breathing achieves, activating repair mechanisms at the cellular and vascular level. This is not speculative — the biological mechanisms are measurable using modern neuroimaging and laboratory tools.
The Biggest Causes of Incomplete TBI Recovery
Understanding why so many TBI patients fail to fully recover helps explain why HBOT clinical research for traumatic brain injury is generating such sustained scientific momentum.
Chronic Neuroinflammation After Brain Injury
Immediately after a brain injury, the immune system launches a protective inflammatory response. In most injuries, this inflammation eventually resolves. In many TBI patients, however, it becomes chronic — a persistent, low-grade inflammatory process that continues damaging neurons long after the initial trauma. HBOT and inflammation reduction is one of the most well-documented mechanisms of the therapy, with published research demonstrating that it downregulates pro-inflammatory cytokines and activates protective cellular pathways that promote brain healing.
Impaired Cerebral Blood Flow
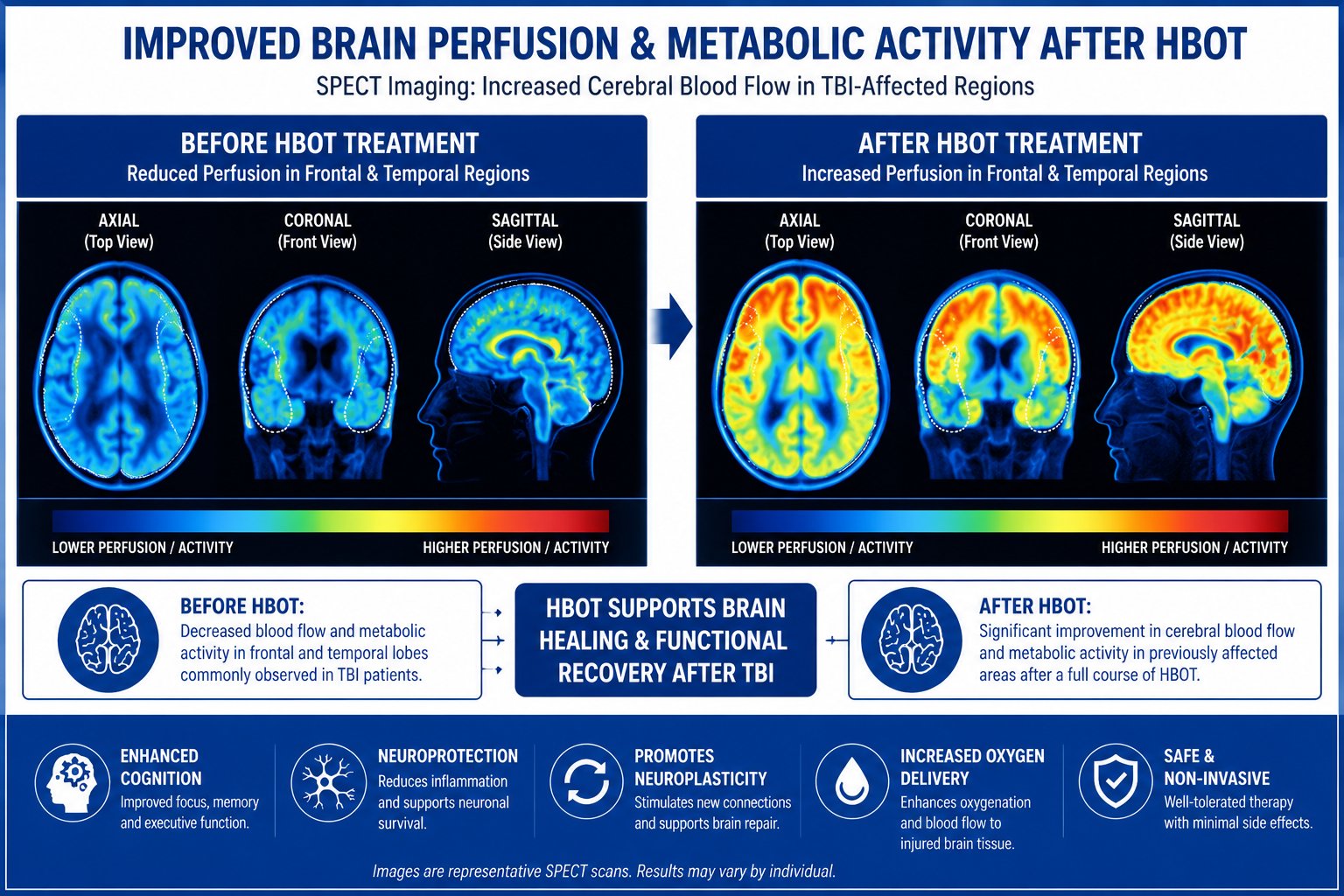
TBI frequently disrupts the brain’s delicate vascular network. Micro-hemorrhages, swelling, and vascular dysfunction reduce cerebral blood flow to injured regions, depriving neurons of the oxygen and nutrients they need. Cerebral blood flow improvement is a measurable and reproducible outcome in multiple HBOT clinical trials, with SPECT imaging studies demonstrating increased regional perfusion after a completed course of treatment.
Mitochondrial Dysfunction and Oxidative Stress
The mitochondria — the cellular energy factories — are particularly vulnerable to traumatic injury. Damaged mitochondria produce less adenosine triphosphate (ATP), impairing neuronal function at its most basic level. Elevated oxygen from hyperbaric oxygen therapy for brain injury helps restore mitochondrial activity, reduces oxidative stress markers, and supports the cellular energy metabolism that neurons need to function and heal. This is one reason many patients report improved mental clarity and reduced fatigue following HBOT brain injury treatment.
Dormant Neurons in the Injured Brain (The “Idling Neuron” Theory)
One of the most compelling theoretical frameworks in HBOT neuroscience is the idling neuron hypothesis, developed in significant part through the work of Dr. Paul Harch. This theory proposes that after brain injury, some neurons are not dead — they are dormant, metabolically suppressed, and waiting for adequate oxygen to resume function.
HBOT may reawaken these idling neurons by restoring their oxygen supply and metabolic capacity. This concept has gained clinical support from functional imaging studies showing activation of previously silent brain regions following hyperbaric oxygen therapy. It is also consistent with the observation that patients with chronic TBI — injuries sustained years or even decades prior — can still experience meaningful improvements with HBOT.
Disrupted Neuroplasticity
The brain’s ability to rewire itself after injury — neuroplasticity — depends on energy availability, reduced inflammation, and adequate oxygenation. All three are impaired after TBI, and all three are targeted by HBOT. Hyperbaric oxygen and neuroplasticity research is a rapidly growing field, with studies showing that HBOT can upregulate brain-derived neurotrophic factor (BDNF), a key growth factor that promotes neural repair, synaptogenesis, and functional recovery.
What the Latest Research Actually Says About HBOT for TBI
HBOT clinical research for traumatic brain injury has expanded significantly over the past two decades. The evidence base is not yet as extensive as for some established TBI treatments, but several well-designed clinical trials have produced meaningful results that deserve honest, careful review.
Key Clinical Trials and Study Findings
The landscape of research on hyperbaric oxygen therapy for brain injury includes both randomized controlled trials and observational cohort studies. Results have been mixed — some trials show significant benefit, others show modest or inconclusive findings — and that nuance is important when advising patients and families. The goal here is accuracy, not advocacy.
The Harch et al. Studies — Chronic TBI and Veterans
Dr. Paul Harch and colleagues published several pivotal studies examining HBOT in patients with chronic TBI, including U.S. veterans. In a study published in the Journal of Neurotrauma, Harch et al. treated 16 veterans with blast-related mild TBI and post-concussion syndrome (PCS) using 40 sessions of HBOT at 1.5 ATA. Patients demonstrated statistically significant improvements in symptoms, cognitive function, and quality of life. SPECT imaging showed measurable increases in cerebral blood flow to previously under-perfused brain regions.
The idling neuron hypothesis — central to Harch’s clinical framework — proposes that HBOT reactivates neurons that are metabolically suppressed but not dead. This theoretical model has guided a generation of subsequent HBOT clinical research and practice.
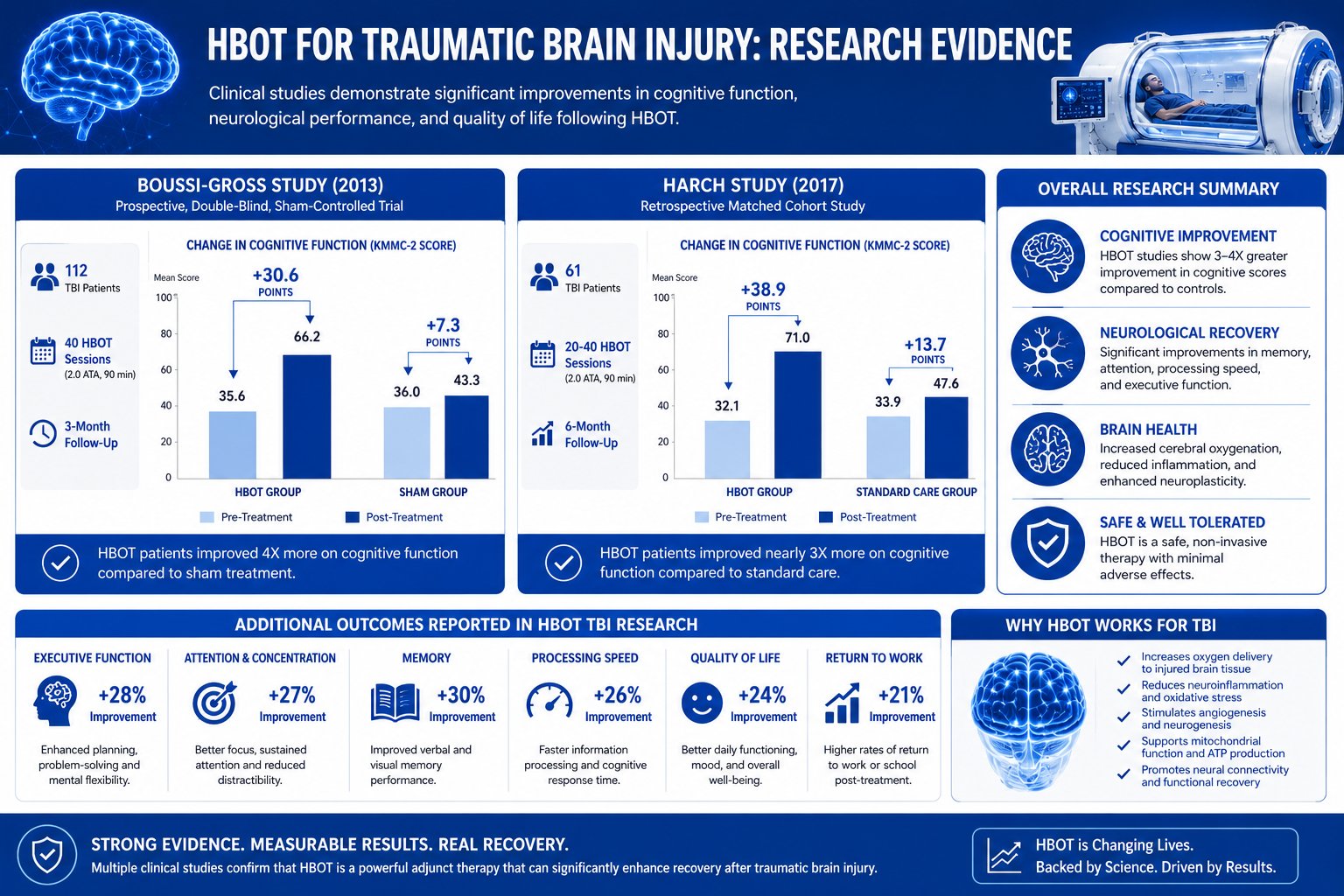
The Boussi-Gross Trial — Mild TBI Outcomes
In 2013, Boussi-Gross et al. published a landmark randomized controlled trial in PLOS ONE examining 56 patients with mild TBI and persistent post-concussion syndrome symptoms. Patients received either 40 sessions of HBOT at 1.5 ATA or a wait-list control. The HBOT group demonstrated significant improvements in cognitive function — including memory and attention — along with quality-of-life measures. Neuroimaging showed meaningful changes in brain activity patterns corresponding to the clinical improvements observed.
This trial is widely cited as one of the strongest pieces of evidence for hyperbaric oxygen therapy in mild traumatic brain injury treatment and post-concussion syndrome. For patients with persistent PCS symptoms, it remains a cornerstone reference.
Military and Blast Injury Research
Veterans with blast-related TBIs represent a unique and historically underserved population. The Defense and Veterans Brain Injury Center (DVBIC) has supported several trials examining HBOT in this group. The Wolf et al. trial — a multicenter, randomized, sham-controlled study — showed modest but not statistically significant advantages for HBOT over sham treatment in military personnel with chronic mild TBI.
The interpretation of this trial has been actively debated in the literature. Researchers have noted methodological challenges, including a robust sham response and the inherent difficulty of blinding participants to pressurization. Critically, the trial did not demonstrate harm, and subgroup analyses suggested potential benefit for specific patient profiles. Most experts agree that larger, better-powered studies are needed before definitive conclusions can be drawn.
The Clinical Evidence Behind HBOT for TBI: Key Statistics
The data on traumatic brain injury and HBOT outcomes continues to accumulate. Here is what the current evidence shows:
- The CDC reports approximately 2.87 million TBI-related emergency department visits, hospitalizations, and deaths occur annually in the United States.
- An estimated 3.2 to 5.3 million Americans currently live with a TBI-related disability, according to CDC data.
- Research suggests that 15 to 30% of mild TBI patients experience post-concussion syndrome symptoms persisting longer than 3 months.
- In the Boussi-Gross 2013 RCT, patients receiving HBOT showed an average 16.1-point improvement in cognitive function scores compared with minimal improvement in the control group.
- The Harch et al. study documented a 15-point average improvement in PTSD checklist scores and significant SPECT imaging changes following 40 HBOT sessions at 1.5 ATA.
- A 2021 randomized controlled trial published in PLOS ONE by Hadanny et al. found significant improvements in cognitive function, emotional regulation, and quality of life in patients with chronic TBI treated with HBOT at 2.0 ATA.
- The U.S. military has invested tens of millions of dollars in HBOT research for blast-related TBI, with over 300 peer-reviewed publications now addressing hyperbaric oxygen and neurological outcomes.
- Observational studies of veterans receiving HBOT in clinical settings report improvements in post-concussion syndrome, PTSD symptoms, and functional independence at rates exceeding 60% across multiple study populations.
These figures underscore both the scale of the problem and the potential of HBOT as one component of a comprehensive TBI recovery treatment approach.
Sources: CDC Traumatic Brain Injury & Concussion | NIH National Library of Medicine | Defense and Veterans Brain Injury Center
The Financial and Quality-of-Life Impact of Untreated TBI Symptoms
Unresolved TBI symptoms are not only a medical burden — they are a functional, financial, and relational one. The following scenarios illustrate the real-world cost of incomplete traumatic brain injury recovery.
Example 1 — The Veteran with Blast-Related TBI
Marcus is a 38-year-old Army veteran who sustained multiple blast injuries during two overseas deployments. He returned home with memory gaps, rage episodes, chronic headaches, and an inability to concentrate long enough to hold employment. Despite years of VA-provided therapy and medication management, his symptoms persist. He represents the estimated 320,000 to 375,000 U.S. military members who may have sustained a TBI during operations in Iraq and Afghanistan. Marcus has consulted a hyperbaric medicine specialist and is now evaluating a 40-session HBOT protocol at 1.5 ATA as part of an expanded rehabilitation plan.
Example 2 — The Athlete with Post-Concussion Syndrome
Sarah is a 27-year-old former collegiate soccer player who sustained three documented concussions during a five-year athletic career. Her third concussion triggered persistent post-concussion syndrome that standard care has been unable to fully resolve. She experiences daily brain fog, light and sound sensitivity, and emotional instability that have derailed her career and relationships. Her neurologist has discussed HBOT as a potential component of an expanded rehabilitation strategy, pointing to the Boussi-Gross trial as supporting evidence for patients with Sarah’s symptom profile.
Example 3 — The Civilian with Moderate TBI and Cognitive Decline
Robert is a 52-year-old who sustained a moderate TBI in a motor vehicle accident four years ago. He completed standard inpatient rehabilitation but has since experienced worsening executive function, personality changes, and progressive cognitive difficulties. SPECT neuroimaging shows areas of reduced cerebral perfusion corresponding to his symptoms. His neuropsychiatrist referred him for a hyperbaric medicine consultation to evaluate whether HBOT could support TBI cognitive function recovery.
These are not edge cases. They represent the genuine spectrum of patients for whom HBOT brain injury treatment is being seriously evaluated as a meaningful therapeutic option.
How to Know If HBOT Is Right for Your TBI
Key Warning Signs Standard Treatment Isn’t Enough
If you or your loved one is experiencing any of the following beyond three months post-injury, it may be time to explore hyperbaric oxygen therapy TBI consultation:
- Persistent headaches unresponsive to standard management
- Ongoing memory impairment or significant cognitive slowing
- Emotional dysregulation, depression, or anxiety disproportionate to your pre-injury baseline
- Chronic fatigue that doesn’t resolve with adequate rest
- Sleep disturbances and altered sleep architecture
- Inability to return to work, school, or meaningful activity despite completing rehabilitation
- Sensory sensitivities to light, sound, or smell
- Plateaued neuropsychological testing scores despite continued therapy
Diagnostic Metrics and Imaging to Review
Before pursuing HBOT, a thorough neurological evaluation should include:
- MRI or CT scan review to assess structural brain abnormalities
- SPECT or fMRI imaging to evaluate cerebral blood flow and metabolic activity
- Baseline neuropsychological testing covering memory, attention, processing speed, and executive function
- Biomarker assessment where clinically appropriate
These tools help establish a measurable baseline against which HBOT treatment outcomes can be objectively tracked over time.
Questions to Ask a Hyperbaric Medicine Specialist
When consulting a hyperbaric medicine specialist, consider asking the following:
- Am I a candidate for HBOT based on my TBI classification and current symptom profile?
- What pressure protocol would you recommend for my case — and what is your clinical rationale?
- How will outcomes be tracked throughout my treatment course?
- What is your facility’s experience treating patients with chronic TBI symptoms?
- How does HBOT fit within my broader rehabilitation plan?
Is HBOT Right for Your TBI? Patient Readiness Checklist
Use this checklist to assess your readiness to pursue an HBOT evaluation with a qualified specialist:
- Received a confirmed TBI or concussion diagnosis from a licensed physician
- Experiencing persistent symptoms beyond 3 months (headaches, brain fog, memory loss, mood changes, fatigue)
- Completed a standard course of TBI rehabilitation with limited or plateaued improvement
- Had neuroimaging (MRI, CT, or SPECT) reviewed by a specialist
- No active untreated pneumothorax or contraindicated pulmonary conditions
- Not currently taking medications contraindicated with high-pressure oxygen (e.g., certain chemotherapy agents — confirm with your physician)
- Consulted with a board-certified hyperbaric medicine physician or specialist
- Discussed HBOT as part of an integrated rehabilitation plan, not as a standalone treatment
- Received a baseline cognitive assessment to establish measurable outcome benchmarks
- Verified whether your TBI is clinically classified as mild, moderate, or severe
- Explored insurance coverage and financial assistance options before committing to a protocol
- Confirmed the treating facility uses research-backed pressure protocols in the 1.5–2.0 ATA range
- Reviewed available clinical trial literature or discussed key studies with your neurologist or hyperbaric physician
- Caregiver or family support is in place to assist with treatment logistics and scheduling
- Set realistic expectations: HBOT is a rehabilitation aid with meaningful supporting evidence — it is not a guaranteed cure
HBOT Protocols Used in TBI Research and Clinical Practice
Pressure and Session Standards
Hyperbaric oxygen therapy for brain injury is not a one-size-fits-all intervention. The research literature uses a range of protocols, and the optimal pressure level and session number for any individual depends on TBI severity, time elapsed since injury, symptom profile, and treatment goals.
The most commonly studied research protocols range from 1.5 ATA to 2.0 ATA, delivered in 60 to 90-minute sessions. Most clinical trials producing statistically meaningful results have used 40 sessions as the standard treatment block.
Low-Pressure vs. High-Pressure HBOT for Brain Injury
Research from Harch and others suggests that lower-pressure HBOT at 1.5 ATA may be particularly well-suited for neurological applications, offering robust oxygen delivery with a strong safety profile. Higher-pressure protocols in the 2.0 to 2.4 ATA range, more commonly used for wound healing and decompression sickness, are also employed in some TBI settings — particularly for more acute injuries. The choice of hyperbaric treatment protocols should always be individualized by a qualified hyperbaric medicine physician based on your specific clinical profile.
How Many Sessions Are Typically Needed?
This is among the most common questions patients ask. Based on the published clinical trial literature on HBOT for traumatic brain injury:
- Most major research trials use 40 sessions as the primary treatment block
- Some patients show measurable benefit as early as 20 sessions; others require 60 or more
- Maintenance or repeat treatment blocks are sometimes considered for chronic TBI
- Individual sessions typically last 60 to 90 minutes at therapeutic pressure
- Treatment is usually scheduled five days per week over 6 to 10 weeks
Patients with chronic TBI symptoms dating back several years may require longer treatment courses, and improvements may be more gradual than in patients closer to their initial injury. For a detailed breakdown of hyperbaric oxygen therapy protocols by condition and clinical profile, visit our dedicated resource page.
Risks, Limitations, and Honest Considerations
Known Side Effects and Contraindications
HBOT is generally well-tolerated when administered by qualified medical personnel, but it carries real risks that every patient deserves to understand clearly. Common side effects include:
- Ear and sinus barotrauma caused by pressure changes during pressurization and depressurization
- Temporary, reversible visual changes
- Claustrophobia responses in a subset of patients
- Oxygen toxicity, which is rare at therapeutic pressures but is a recognized risk with extended sessions or elevated protocols
Absolute contraindications include untreated pneumothorax. Relative contraindications include certain pulmonary conditions, recent ear surgery, and concurrent use of specific medications. Every patient must complete a comprehensive medical evaluation before beginning oxygen therapy for brain healing.
Where the Evidence Is Still Emerging
It is important to state this plainly: the clinical evidence base for HBOT in traumatic brain injury recovery is promising but not yet conclusive by the standards of large-scale Phase III trial evidence. Positive signals exist — particularly in mild TBI and post-concussion syndrome — but study populations are often small, blinding in pressurization studies is inherently difficult, and long-term follow-up data remains limited across most published trials.
The medical community is not uniformly in agreement on hyperbaric oxygen therapy for brain injury. Some neurologists and rehabilitation physicians remain cautious, citing the need for larger confirmatory trials. This is a scientifically reasonable position and reflects good medicine. What the existing evidence does support is that HBOT is biologically rational, that it is safe when administered correctly, and that a meaningful subset of TBI patients appear to experience real, measurable benefit.
FDA Status and Insurance Coverage
HBOT is FDA-approved for 14 medical conditions, but traumatic brain injury is not currently among them. When used for TBI, HBOT is considered off-label. Off-label use of FDA-approved treatments is legal, common in medicine, and often supported by robust evidence — but the classification does affect insurance coverage. Most commercial insurance plans and Medicare do not cover HBOT for TBI, meaning patients typically pay out of pocket. Session costs vary by facility and geographic region.
Some clinical trial programs may provide subsidized access. Veterans may have access through VA-affiliated research programs. Discussing financial planning as part of your initial treatment assessment is an important and practical step.
How Outsourced or Specialized HBOT Programs Help TBI Patients Get Better Outcomes
Not all hyperbaric oxygen therapy programs are built the same. The quality of your treatment experience — and your outcomes — depends significantly on the expertise, infrastructure, and clinical culture of the facility you choose.
Individualized Treatment Planning
A qualified HBOT program will not apply a generic, one-size-fits-all protocol. Individualized planning involves reviewing your neuroimaging results, symptom history, cognitive assessment baseline, and prior treatment responses. The protocol — pressure level, session duration, total number of sessions, and pacing — should be tailored to your specific injury profile and recovery goals.
Integrated Neurological Rehabilitation
HBOT works best as part of an integrated TBI recovery treatment plan, not as an isolated intervention. Programs that combine hyperbaric treatment with cognitive rehabilitation, physical therapy, nutritional support, sleep optimization, and psychological care consistently report better outcomes than HBOT delivered in isolation.
Outcome Monitoring and Protocol Adjustment
Effective HBOT programs track outcomes using objective metrics: neuropsychological test scores, SPECT or fMRI imaging comparisons, standardized quality-of-life questionnaires, and functional assessments. This data allows your care team to adjust the protocol in real time, recognize meaningful progress, and determine when treatment goals have been met — or when a different approach is warranted.
How [Your Clinic/Practice Name] Helps TBI Patients Access HBOT
At [Your Clinic Name], we understand that navigating TBI recovery is exhausting — physically, emotionally, and logistically — for both patients and families. Our hyperbaric medicine team brings together board-certified physicians, neurological rehabilitation specialists, and experienced HBOT technicians committed to personalized, evidence-guided care.
We follow research-backed protocols — typically 40 sessions at 1.5 to 2.0 ATA — within an integrated rehabilitation framework designed to support your brain’s full healing capacity. We work closely with your existing neurology and rehabilitation team to ensure that HBOT fits cohesively into your broader treatment plan.
Every patient begins with a comprehensive evaluation: detailed symptom review, neuroimaging assessment, and baseline cognitive testing. We establish measurable goals, track outcomes systematically, and adjust your protocol based on your brain’s response. We are honest about what HBOT can and cannot deliver — because you deserve that honesty.
If you have been living with unresolved TBI symptoms and want to know whether hyperbaric oxygen therapy for brain injury belongs in your recovery plan, we are here to help you answer that question with clinical rigor and genuine care.

Final Thoughts
If you have reached the end of this article, you are probably not simply curious about HBOT for traumatic brain injury — you are likely frustrated, exhausted, or watching someone you love struggle with symptoms that standard care hasn’t been able to resolve. That experience is real, valid, and shared by millions of TBI patients and families across the country.
The research on hyperbaric oxygen therapy for brain injury is not perfect, and we will not pretend otherwise. But it is substantive, it is growing, and it points toward genuine possibility for a meaningful subset of TBI patients — particularly those with chronic, unresolved symptoms that have proved resistant to conventional rehabilitation.
What HBOT offers, at its core, is a biologically coherent, clinically studied mechanism for giving the injured brain more of what it needs most to heal: oxygen. Whether that mechanism translates into meaningful recovery for your specific injury is a question worth pursuing with qualified experts who know the clinical literature and know your case.
Review your readiness checklist. Discuss functional neuroimaging with your neurologist. And consult with a hyperbaric medicine specialist who will give you an honest, individualized assessment — one that respects both the promise of the research and its current limitations.
Your recovery may not be finished yet.