
A Step-by-Step Guide to E/M Coding for Internal Medicine Physicians
If you’re an internal medicine physician or practice manager, you already know that getting E/M coding right isn’t optional — it’s essential. Evaluation and Management (E/M) codes drive the bulk of your revenue, and even small, consistent errors compound into serious financial and compliance problems over time. Whether you’re dealing with claim denials, uncertain about 2026 documentation standards, or just trying to understand what your billing team is doing with your charts, this guide is for you.
At TMS Billing, we work every day with internal medicine practices across the country. Our Internal Medicine Billing and Coding Support team has built this step-by-step walkthrough around real coding scenarios, 2026 guidelines, and the most common questions we hear from physicians just like you. E/M coding for internal medicine physicians doesn’t have to feel like a black box — and it won’t, after you read this.
Let’s walk through it.
Why E/M Coding Is the Backbone of Internal Medicine Billing
Internal medicine practices generate income primarily through office visits, hospital care, and chronic disease management — all of which are billed using E/M codes. For most internal medicine physicians, E/M services represent the majority of professional fee revenue. That alone makes coding accuracy a top business priority.
But the rules governing these codes are detailed, regularly updated, and carefully scrutinized by payers and regulators alike. The AMA and CMS overhauled E/M guidelines significantly starting in 2021, eliminating the old history and physical exam bullet-counting approach in favor of a framework built around Medical Decision Making (MDM) and total time. Those changes continue to define how E/M documentation requirements for internal medicine are applied in 2026.
Physicians who don’t stay current with internal medicine physician billing guidelines risk:
- Underbilling for complex visits — a pattern called downcoding
- Overbilling through unsupported high-level claims — upcoding — which invites audits
- Triggering payer recoupments or OIG scrutiny
- Losing thousands of dollars annually in legitimate reimbursement they’ve simply never captured
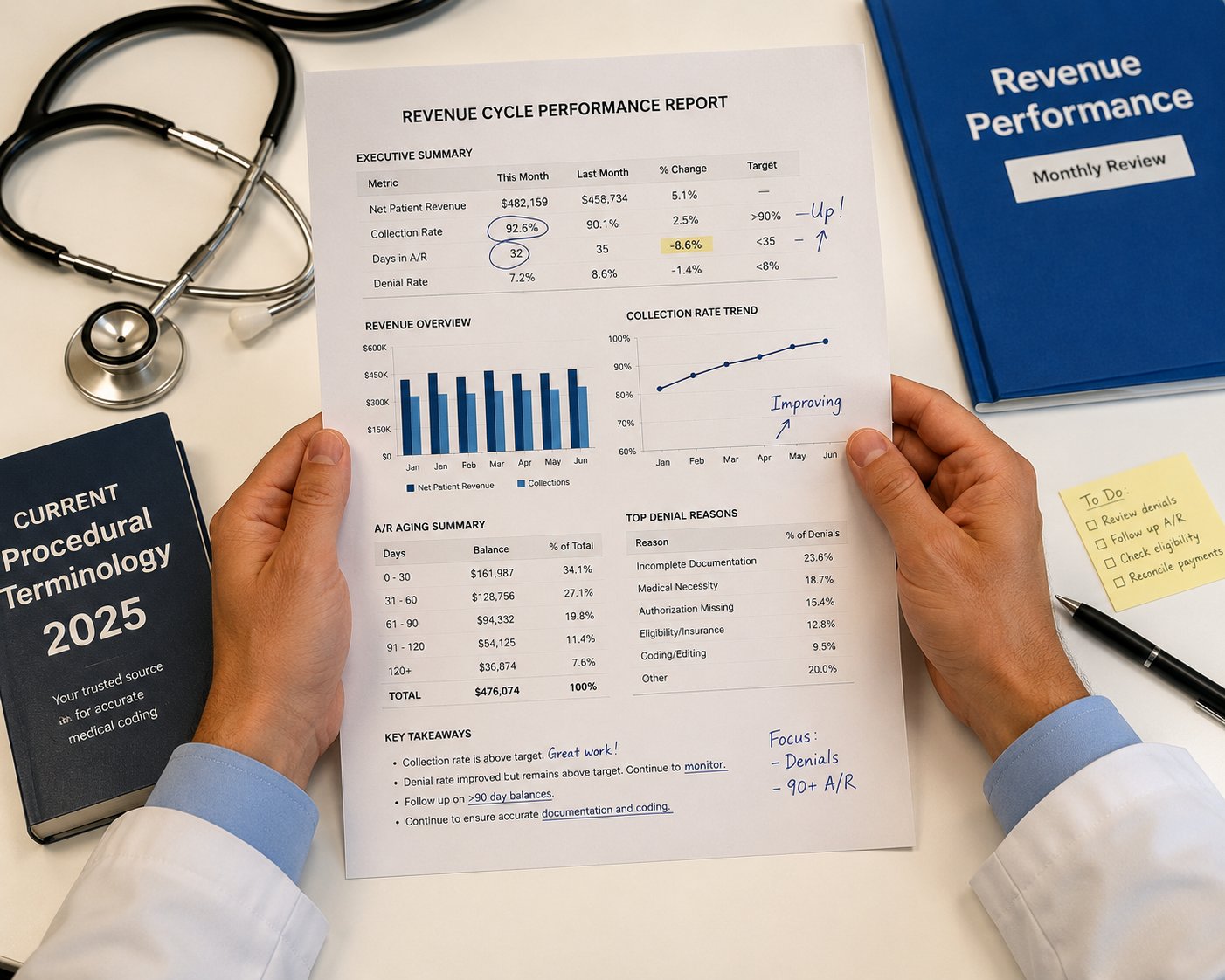
According to MGMA physician revenue cycle benchmarking data, even modest improvements in coding accuracy translate to measurable revenue gains across a practice. Getting E/M coding right isn’t just a compliance issue — it’s a financial one.
Understanding the E/M Coding Framework in 2026
Before you can code correctly, you need a solid grasp of how the current framework actually works. In 2026, every outpatient E/M visit is coded using one of two pathways: Medical Decision Making or Total Time. The old system — counting history elements, physical exam bullets, and organ systems — is gone. What’s here now is more clinically intuitive, but it still demands precision and documentation discipline.
1. The Two Pathways — MDM vs. Total Time
Medical Decision Making (MDM): This pathway evaluates the complexity of the clinical problems you’re addressing, the amount and complexity of data you’re reviewing, and the risk associated with your management decisions. Each element has defined tiers, and your documentation must support whatever level you assign.
Total Time: This pathway lets you code based on the total time you spend on the date of the encounter — including non-face-to-face work such as reviewing outside records, ordering and reviewing tests, and coordinating care with other providers. Time-based billing for internal medicine in 2026 is especially useful for visits involving complex care coordination, lengthy patient counseling, or substantial documentation burden.
You choose one pathway per encounter — whichever best reflects the work and is better supported by your notes.
2. How to Select the Right Level of Service
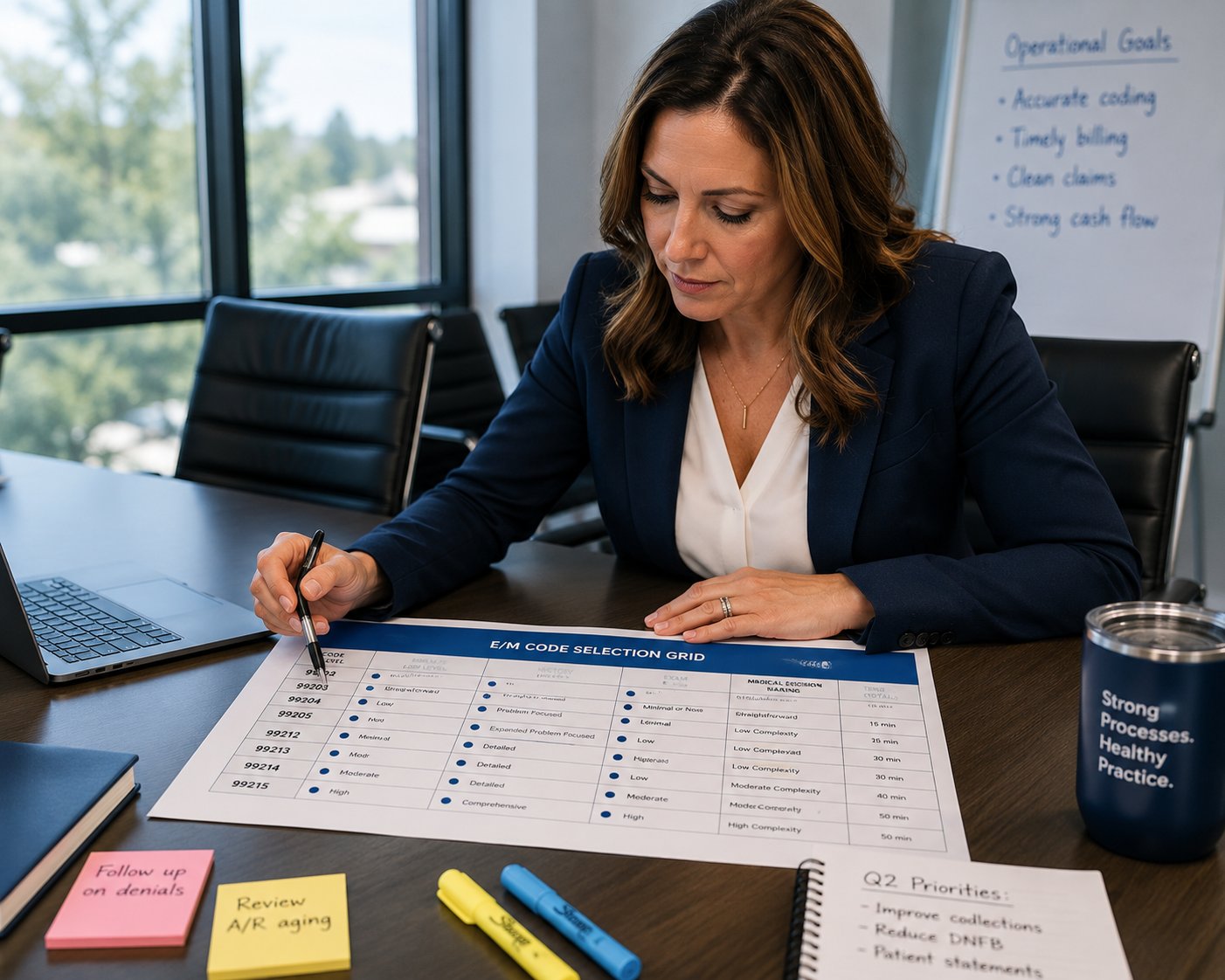
E/M code selection criteria require that your documentation genuinely support the level you’re billing. For outpatient office visits, the relevant CPT codes are:
New Patients: 99202 (Straightforward), 99203 (Low), 99204 (Moderate), 99205 (High complexity)
Established Patients: 99211 (Minimal), 99212 (Straightforward), 99213 (Low), 99214 (Moderate), 99215 (High complexity)
Selecting the appropriate level of service in internal medicine coding means matching your actual clinical work to the code — not defaulting to a “safe” mid-level out of habit, and not routinely billing the highest code without documentation support. Both extremes cost you.
3. New Patient vs. Established Patient Coding Rules
A patient is “new” if they haven’t received professional services from the physician, or from any physician in the same group practice of the same specialty, within the past three years. This distinction determines which code series applies and therefore which reimbursement rates you’ll receive.
In a busy internal medicine group, this distinction gets blurry — and coding it incorrectly, consistently, is one of the common E/M coding mistakes internal medicine physicians make that we catch during audits. Know your patient history before you code.
Step-by-Step E/M Coding for Internal Medicine Office Visits
Here’s the step-by-step E/M coding guide for internal medicine doctors that we apply to client charts every day.
Step 1 — Document the Presenting Problem Accurately
Everything starts here. “Follow-up” is not a presenting problem. “Follow-up for uncontrolled Type 2 diabetes with A1C of 10.2% and new peripheral neuropathy symptoms” is a presenting problem that anchors high-complexity MDM.
Specificity at this stage sets the foundation for every coding decision that follows. The more precise your presenting problem, the more clearly your documentation justifies the complexity of care you’re delivering.
Step 2 — Choose MDM or Time as Your Basis
Once the encounter is documented, decide which pathway gives you the most accurate code for the work you actually did.
MDM-based coding is typically the stronger pathway when the visit involved:
- Multiple chronic conditions being actively managed
- Review of external records or independent interpretation of diagnostic results
- High-risk treatment decisions — starting anticoagulation, managing polypharmacy, coordinating specialist referrals
- Prescription drug management with documented monitoring risk
Time-based billing becomes the better choice when you can clearly document total time spent on the date of service — and that time pushes you into a higher E/M level than MDM alone would support.
Real-world example: Dr. Amara sees an established patient with uncontrolled hypertension, Stage 3 CKD, and newly diagnosed prediabetes. She reviews labs from an outside facility, spends time on the phone coordinating with nephrology, counsels the patient on dietary changes, and adjusts two medications. Her total time on the date of service is 47 minutes. She can support a 99215 via MDM — high-complexity problems, external data review, prescription management risk — or via time (40+ minutes = 99215 for established patients). She documents both so her claim is defensible either way.
That’s medical decision making MDM in internal medicine applied correctly.

Step 3 — Assign the Correct CPT Code
With your pathway determined, assign the code that matches your documented complexity. Don’t default to 99213 for every established patient. If your documentation supports 99214 or 99215, bill it — you’ve earned it, and not billing it is real revenue loss compounded over hundreds of visits per year.
For new patients, undercoding is especially common. Many physicians bill 99203 or 99204 when the complexity of the first visit clearly supports 99205. Office visit coding in internal medicine for new patients often involves more extensive data review, more complex problem assessment, and higher management risk than the physician gives themselves credit for.
This is also where CPT codes for E/M visits in internal medicine intersect with medical coding compliance for physicians. The code must be supported by the note — not just by the care delivered, but by the care documented.
Step 4 — Match ICD-10 Codes to the Clinical Picture
ICD-10 coding accuracy affects more than compliance. It directly influences:
- Medical necessity determinations by the payer
- How quickly your claim is adjudicated
- Your risk adjustment calculations under value-based care contracts
- Whether your claim survives audit review
Use the most specific ICD-10 codes your documentation supports. If your patient has Type 2 diabetes with diabetic chronic kidney disease, don’t code only E11.9 — that’s underspecified. Code E11.65 (Type 2 diabetes mellitus with hyperglycemia) alongside N18.3 (Chronic kidney disease, Stage 3) where the documentation supports it.
Mismatched ICD-10 and CPT codes are among the most consistent coding errors in internal medicine claims we see in denial queues. A high-complexity E/M with a low-acuity diagnosis flags payer systems immediately.
Step 5 — Review Before Submission
Before any claim goes out, it should pass through a review — by a coder, a billing specialist, or at minimum a trained front-office reviewer who understands both the clinical note and the coding criteria. Ask these questions:
- Does the documented MDM support the level billed?
- If using time, is total time explicitly documented in the note?
- Are ICD-10 codes as specific as the clinical picture allows?
- Do the CPT and diagnosis codes tell a coherent story about the patient’s condition?
A physician billing audit — even a monthly self-audit of a random chart sample — catches patterns before they become a payer problem.
Common E/M Coding Mistakes Internal Medicine Physicians Make
Knowing how to correctly code E/M visits for internal medicine in 2026 means knowing what not to do just as clearly. These are the patterns we see repeatedly.
Upcoding and Downcoding — Both Are Costly
Most physicians think of upcoding as the primary compliance risk, and it is — billing higher than what documentation supports invites audits, recoupments, and potentially fraud referrals. But downcoding is equally damaging, just quietly. A physician who habitually bills 99213 for encounters that document 99214-level complexity loses tens of thousands of dollars per year across a full practice panel.
Poor MDM Documentation
Medical decision making MDM in internal medicine requires documenting all three elements: the number and complexity of problems, the amount and complexity of data reviewed, and the risk of management. Physicians routinely address all three in practice — but don’t document them explicitly enough for a coder or payer reviewer to map them to the coding criteria.
The fix isn’t longer notes. It’s smarter notes — structured to make complexity apparent without adding unnecessary verbiage.
Mismatched ICD-10 and CPT Codes
ICD-10 coding accuracy matters for claim integrity. Submitting a high-level E/M code paired with a low-acuity diagnosis is a red flag that payers notice and act on. These mismatches generate denials, records requests, and — in audit scenarios — findings that require recoupment.
Ignoring Time-Based Billing Opportunities
Time-based billing for internal medicine in 2026 is underused. Many physicians don’t realize that documenting 35 minutes of total time on an established patient visit qualifies them for a 99214 even when their MDM documentation alone might not fully support it. If you’re investing significant time in patient care, don’t leave that billing pathway unexplored.
How Outsourcing Helps Internal Medicine Physicians Reduce Coding Errors
How outsourcing helps internal medicine physicians reduce coding errors is something we talk about often — because the difference between in-house and outsourced coding in a specialty like internal medicine is measurable and consistent.
What Certified Coders Do Differently
A certified coder specializing in internal medicine reads the entire clinical picture: the presenting problem, the MDM elements, the ICD-10 specificity, and the interaction between diagnosis and procedure codes. Outsourced medical coding accuracy depends on specialty-specific knowledge — not generalist coders rotating between specialties. Internal medicine documentation patterns, risk-adjustment nuances, and common presenting problems require familiarity that only comes with focus.
Real-Time Coding Audits and Feedback
One of the highest-value things outsourced coding services for internal medicine can provide is education, not just code assignment. When your coding partner conducts regular chart audits and delivers physician-level feedback on documentation gaps, your practice improves over time. Physicians develop better note habits. Patterns of undercoding get corrected. Medical coding compliance for physicians becomes a practice-wide culture rather than a billing department concern.
A physician billing audit performed by an external team also removes the conflict-of-interest problem inherent in auditing your own work.
Staying Compliant With 2026 Coding Updates
E/M guidelines don’t stay still. CMS publishes annual updates to E/M documentation and coding policies through the Physician Fee Schedule process, and the AMA releases CPT revisions that affect code definitions and usage. Staying current is a genuine full-time task that most physicians and practice managers simply can’t prioritize alongside clinical care.
Outsourced coding teams track these updates continuously, incorporate payer-specific policy changes, and ensure your practice’s coding reflects current standards — not last year’s.
E/M Coding for Hospital Visits, Consultations, and Telehealth
Office visit coding gets the most attention, but internal medicine physicians bill across a wide range of E/M service types — and the rules differ in important ways.
Hospital visits: Initial inpatient hospital care uses 99221–99223; subsequent inpatient care uses 99231–99233; discharge day management uses 99238–99239. These codes still rely on MDM complexity or total time, but the complexity thresholds are calibrated to inpatient acuity.
Consultations: CMS doesn’t recognize consultation codes (99241–99245) for Medicare — inpatient consults bill using subsequent hospital care codes or initial hospital care codes instead, depending on the situation. However, many commercial payers do recognize consultation codes. Knowing your payer mix is essential here. Using the wrong code for a consultation is an automatic denial with some payers.
Telehealth: Since the expanded telehealth waivers, E/M coding for telehealth visits in internal medicine has become a permanent feature of practice. In 2026, most standard outpatient office visit codes apply to telehealth encounters, but documentation must include the patient’s physical location at the time of the visit. The AMA’s CPT telehealth and E/M coding guidelines provide regularly updated guidance that your billing team should be applying consistently.
How TMS Billing Supports Internal Medicine Physicians With E/M Coding
At TMS Billing, E/M coding for internal medicine physicians is our core focus — not a side service. Our team works exclusively with internal medicine practices, which means we understand your patient population, your common presenting problems, and the documentation patterns that distinguish a 99213 from a 99215 in your specialty.
Here’s what working with TMS looks like in practice:
- Chart-level review: Every encounter gets reviewed against the MDM criteria and time documentation before submission. Discrepancies are flagged and resolved before the claim goes out.
- Denial management: When payers deny claims, we work them — appealing with supporting documentation, correcting and resubmitting, and tracking denial patterns to address root causes.
- Physician-level reporting: You receive regular reports on your coding distribution, denial rates, and revenue performance — so you’re never in the dark about where your practice stands.
- Ongoing compliance monitoring: We track 2026 coding updates, payer policy shifts, and audit trends as they happen, and we incorporate them into your billing workflow proactively.

The best coding and billing support for internal medicine physicians comes from a team that knows the specialty deeply. If you’re tired of wondering whether your coding is right — or watching revenue slip through errors that shouldn’t happen — this is what Internal Medicine Medical Billing Services from a specialty-focused billing partner looks like.
Internal Medicine Billing and Coding Tips for Physicians and Practice Managers
A few practical reminders worth keeping close — regardless of your practice size or billing setup:
- Document the complexity you’re managing, not just the tasks you completed. Your note should make clinical complexity obvious to an outside reviewer — whether that’s a coder, an auditor, or a payer’s medical director.
- Don’t rely solely on EHR auto-templates. Most EHR systems don’t automatically populate MDM elements. You still need to document your clinical reasoning explicitly.
- Track your denial patterns monthly. If the same denial reason keeps appearing, it’s a signal — a coding issue, a documentation gap, or a payer policy you’re not accounting for.
- Use time-based coding when it serves you. If you’re consistently spending 35–45 minutes on established patient visits, check whether documenting and billing total time gets you to a higher supported level.
- Audit yourself. Pull 10 random charts per month and trace the coding logic from note to claim. This habit catches errors early and builds real fluency in E/M code selection criteria.
- Know how your payer contracts affect your coding. Internal medicine physician billing guidelines vary by payer. Medicare rules differ from Medicaid, which differ from BCBS or Aetna contracts. One-size-fits-all coding assumptions produce preventable errors.
Applying these habits consistently is what separates practices that merely bill from practices that consistently capture the revenue they’ve earned.
Final Thoughts
E/M coding for internal medicine physicians is an area where precision pays — literally. Every encounter coded correctly supports your revenue, strengthens your compliance posture, and builds a documentation record that holds up under scrutiny. Every recurring error costs money, wastes time, and creates risk your practice doesn’t need to carry.
The step-by-step E/M coding guide for internal medicine doctors outlined here reflects the process we apply at TMS Billing every day across hundreds of physician encounters. It’s not theoretical — it’s the actual workflow that helps internal medicine practices capture earned revenue and avoid the common mistakes that quietly drain profitability.
If you’re ready to stop second-guessing your coding, cut your denial rate, or simply get a clear picture of where your billing stands, we’d genuinely like to help. A free coding audit from our team takes the guesswork out of it — you’ll see exactly where your practice has room to improve and what better performance actually looks like.
Reach out to our Internal Medicine Billing and Coding Support team today. No pressure — just an honest, experienced conversation about your coding performance and how to make it work harder for your practice.